Brain Science Through the Lens of Brain-Computer Interfaces

What Is a Brain-Computer Interface, Where Did It Come From, and Where Is It Going?
At the 2014 Brazil World Cup opening ceremony, a paralyzed former football player used brain-computer interface (BCI) technology to control an exoskeleton and successfully completed a two-second kickoff. Those two seconds, a decade ago, have long been considered a milestone for BCI technology. Through BCI, this former athlete reclaimed the confidence that originated on the pitch. Amid the noisy stadium environment, the BCI demonstrated its technical potential for stable control.
The development of BCI technology was no accident — it is the result of interdisciplinary innovation and integration. From neuroscience and brain science to materials science and psychology, and onward to computer science, BCI has become a frontier where multiple disciplines converge. In developing BCIs, we are not only clearing the barriers between brain and machine but also gradually unveiling the mysteries of the brain while advancing human intelligence.
In this industry research report, we will examine BCI classifications, scientific principles, development trajectories, and commercialization pathways to analyze the innovation opportunities and directions in this field. This is the third brain science-related report we have published; our previous two reports, released in 2021 and 2022, focused on the origins and research methodologies of brain and cognitive science, as well as the new tools and therapies that have emerged.
We continue to monitor entrepreneurial and investment opportunities in brain science and look forward to partnering with more innovative companies to unlock more unknown territories.
Reader Giveaway: What changes do you expect BCI technology to bring to daily life? Leave a comment below — we'll randomly select five readers to each receive a copy of Brain-Computer Interfaces: From Science Fiction to Reality.

01 What Is a Brain-Computer Interface, and What Can It Do for Humanity?
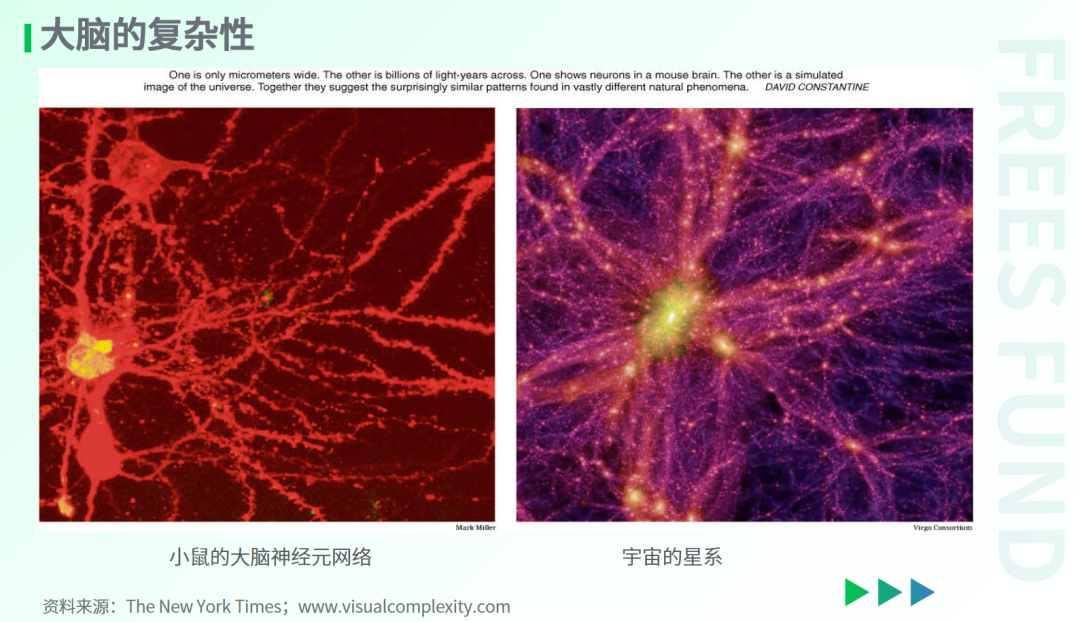
The human brain is an extraordinarily complex structure with 86 billion neurons and over a trillion neural connections — the most powerful "computer" known to date. The New York Times once published two photographs: one of a mouse's neural network, the other of galaxies in the universe. The similarity was striking. The brain and the cosmos appear to share the same connectivity structure. Hence, the human brain has been called "a three-pound universe."
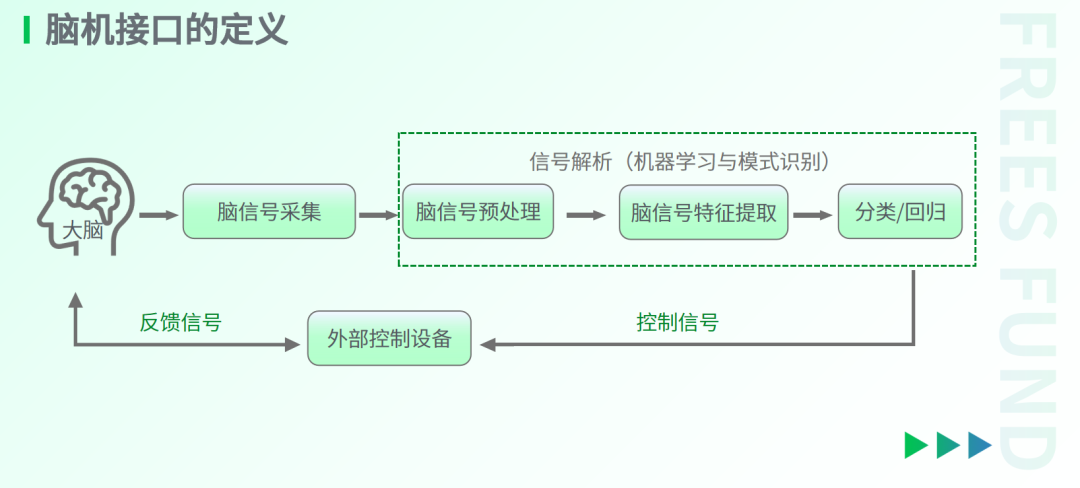
How do we study the brain's complex connectivity, observe and interpret its activity, and even modulate it? Brain-computer interfaces offer a new approach by building a "bridge" for interaction between the human brain and external devices.
Specifically, the "brain" in BCI refers to the human brain and central nervous system, while the "computer" refers to external devices — robotic arms, keyboards, mice, cameras, even drones, electronic skin, and other apparatuses. A BCI can translate the brain's intentions into commands to control devices, or conversely, write information into the brain through external devices.
BCI research may seem like science fiction, but it actually addresses fundamental questions: Can the brain's intentions be decoded? Can knowledge in the brain be directly read or even "downloaded"? The application potential is equally tantalizing. Could BCIs make us smarter? Enable true multitasking?
From a broader, longer-term perspective, the value of BCIs lies in liberating communication from dependence on language or physical movement — using the brain itself as the medium to connect with the outside world.
Humans cannot communicate faster than the speed of their own language. Yet the knowledge and experiences in our brains are often far richer than what language and behavior can express, and our brains are capable of adapting through training to faster reading (information input) and writing (information output) speeds.
A more concrete comparison: while the human brain has greater computing power than a computer with equivalent energy consumption, traditional language and text output is relatively slow — roughly 40–60 bits per second. Computer information transmission far exceeds this, reaching millions of bits per second, roughly 200,000 times faster than language.
BCIs could break the constraints of traditional language and enable more efficient transmission of information from the brain. This new form of communication will generate enormous value across multiple dimensions: answering fundamental questions in neuroscience, intervening in brain diseases, and enhancing the efficiency of learning and interaction.
02 Why Focus on Brain-Computer Interfaces Now?
The concept of brain-computer interfaces was formally proposed in 1973 — more than half a century ago. Neuralink, the iconic BCI company, was founded in 2016 — seven years ago.
If seven years ago the BCI industry was primarily centered on materials innovation and interpretation of brain electrophysiological signals, the field has now shifted toward product development and clinical applications.
On the product and clinical front, Neuralink received clinical trial approval from Health Canada in November 2024 and began recruiting volunteers to evaluate the preliminary functionality of its BCI in "helping quadriplegic patients control external devices with their thoughts." In China, a BCI product co-developed by Tsinghua University professor Hongbo Liu's team and industry partners became the country's first BCI product to enter the innovative medical device special review process in August 2024.
On the industry front, the International Brain-Computer Interface Conference, co-hosted by the Tianqiao and Chrissy Chen Institute and the BCI Society, was held in Shanghai in December 2024 — the first time in its 25-year history that this top-tier international academic conference was held in Asia.
Regarding industry standards, in May 2024, China's Cyberspace Administration and two other departments issued the Action Plan for Information Technology Standardization Construction (2024–2027), emphasizing the advancement of BCI standardization research and the development of key technical and application standards for input-output interfaces, brain information encoding and decoding algorithms, and BCI information security and privacy protection. In June 2024, the Ministry of Science and Technology released Ethical Guidelines for Brain-Computer Interface Research, defining and categorizing terminology in BCI technology and clarifying potentially ambiguous concepts in ethics review work. This marked China's first dedicated ethical guidance document for BCI research.
Why is BCI so hot right now, and why should we pay attention?
From a technology evolution standpoint, BCI is an interdisciplinary field integrating the latest advances in brain science, materials science, artificial intelligence, and more — progress in each of these individual disciplines will drive BCI development. Since 2000, BCI patents spanning various disciplines have grown significantly.
From a research perspective, brain science has progressed from a stage of "not knowing where to begin" to one of "having some tools, but still needing to go deeper." Invasive BCI technology is expected to enable observation from single neurons to millions of neurons, helping us better understand micro- and mesoscale brain activity. From a dimensional standpoint, electrodes are currently the only means to observe the human brain from micro to mesoscale. BCIs will bring new conclusions to unraveling the puzzles of brain science.
In clinical applications, BCIs offer new hope for treating certain diseases that have no pharmaceutical solutions. For instance, BCIs could alleviate the困境 of slow drug development and lack of available treatments for central nervous system (CNS) diseases by providing a method to evaluate CNS drug effects in the brain. Specifically, clinical BCI applications in humans could intervene in spinal cord injuries, aphasia caused by damage to language areas, and other conditions with no current medical cure.
In terms of market size, the BCI market is growing rapidly. According to data from Precedence Research and Market.US, the global BCI market exceeded $2 billion in 2023 and is projected to grow at a compound annual growth rate of 17%, surpassing $10 billion by 2033. According to a thematic report published by QbitAI, China's comprehensive BCI market could reach 125 billion yuan by 2040, with device market size potentially exceeding 50 billion yuan.
Additionally, given intensifying international competition and the sensitivity of brain data, developing autonomous and controllable BCI electrode materials, devices, and algorithms is necessary to advance China's domestic BCI industry.
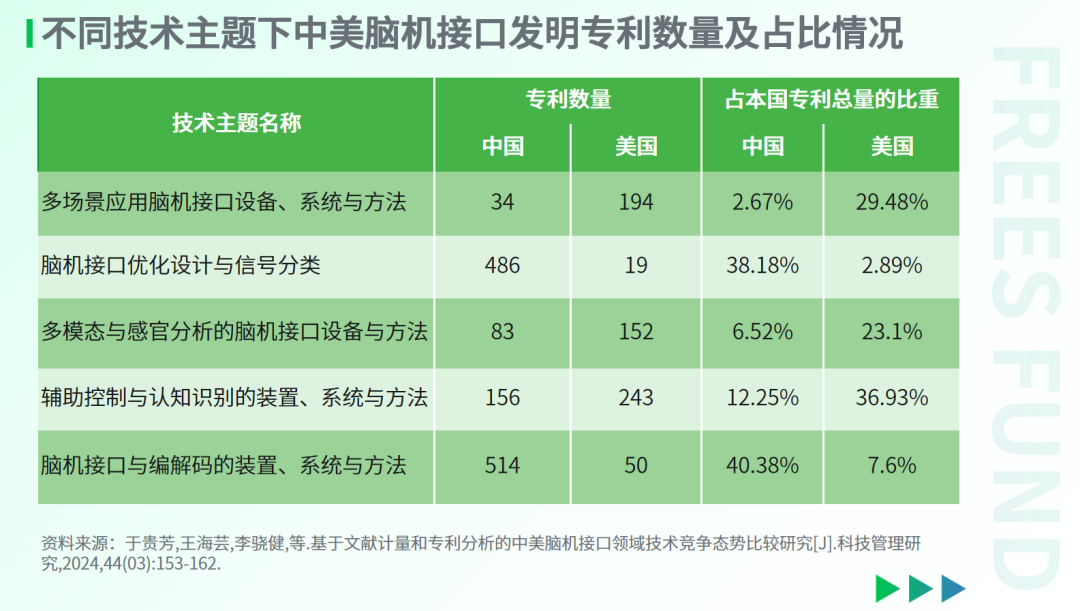
As early as November 2018, the U.S. Department of Commerce's export control framework for 14 categories of key technologies and related products included items directly related to BCIs, such as neural control interfaces, mind-machine interfaces, and direct neural interfaces. In terms of patent volume, China's advantages in BCI technology development are primarily in EEG data encoding/decoding and BCI optimization design, while the U.S. focuses more on areas directly related to application scenarios, such as multi-scenario applications and multimodal and sensory analysis methods.
03 What Types of Brain-Computer Interfaces Exist?
I. Based on Physical Interaction with the Brain
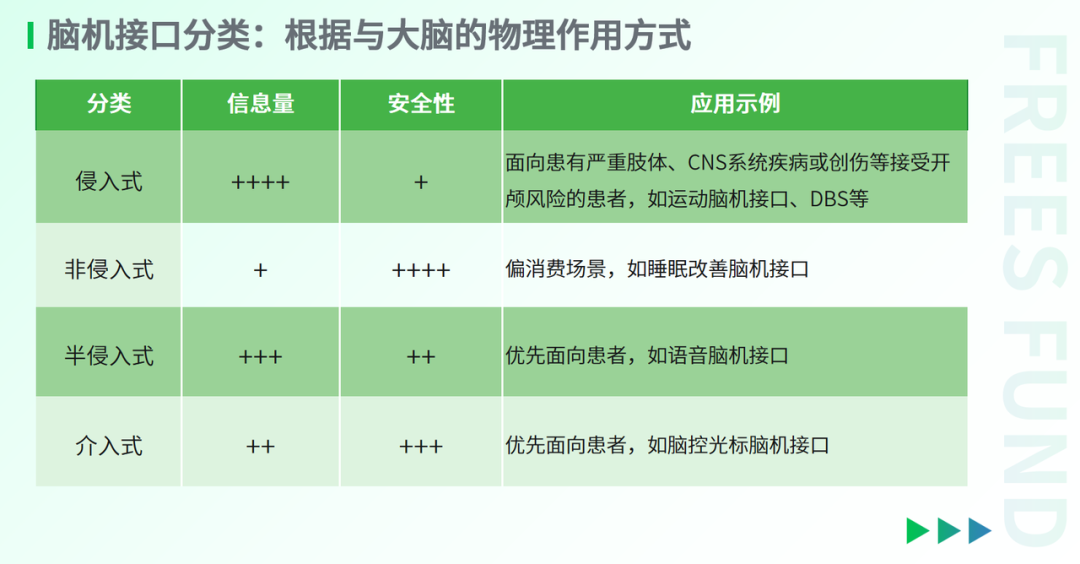
Based on their physical interaction with the brain, BCIs can be classified into four types: invasive, non-invasive, semi-invasive, and interventional. We can use the perspective of "exploring celestial bodies" to understand how different types of BCIs investigate the human brain.
1. Invasive
Invasive BCIs are like landing on a planet to collect soil and specimens for study. They involve implanting electrodes directly into the brain to record or modulate neuronal electrical activity. The recorded data typically includes single-neuron spike discharges and aggregate potential changes from multiple neurons firing within a local region. Compared to other BCI types, invasive BCIs yield the most precise signals and the richest information through in-situ acquisition. From a clinical translation standpoint, invasive BCIs are currently the only means of recording and even regulating activity from single neurons up to millions of neurons, spanning micro- to mesoscopic scales. Their development is considered essential for decoding the brain and treating major neurological disorders.
On the other hand, invasive BCIs require craniotomy for implantation, are often difficult to remove afterward, and the implants must demonstrate long-term biocompatibility. Consequently, progress in this field has been relatively slow. Clinically, researchers carefully weigh risks against benefits, prioritizing BCIs for patients with severe motor disabilities or brain diseases.
Currently, "brain pacemakers" that collect neural signals and deliver electrical stimulation based on abnormal activity patterns can be considered commercially available invasive BCIs. They are primarily used to treat Parkinson's disease, essential tremor, and epilepsy. By contrast, invasive BCIs capable of broader brain signal interpretation remain in clinical trials. The Utah array, for instance, is a commonly used invasive BCI electrode that received FDA clinical trial approval in 2004. Up to 100 hair-thin electrodes are arranged on a metal substrate smaller than a one-yuan coin, enabling simultaneous recording from hundreds of neurons. To date, fewer than 40 subjects worldwide have received Utah array implants.
2. Non-Invasive
Non-invasive BCIs are like observing a planet from afar. They typically collect or modulate brain activity signals from the scalp surface or without physical contact. Common signal acquisition methods include electroencephalography (EEG), magnetoencephalography (MEG), and blood-oxygen-level-dependent (BOLD) signals; common intervention methods include transcranial electrical stimulation, transcranial magnetic stimulation, and even sensory stimulation.
This approach requires no cranial surgery. Users typically need only wear a helmet or forehead patch, or sometimes no direct contact at all, making it safer and more convenient for clinical use. However, because the skull shields and distorts signals, non-invasive BCIs offer limited spatial resolution and relatively constrained information bandwidth, restricting them to simpler control tasks for now.
Given high user acceptance, non-invasive BCIs have found favor in consumer-oriented applications first, and their commercial potential should not be underestimated. For example, NeuroX (脑陆科技) previously released SleepUp, a sleep patch for sleep monitoring and mild sleep assistance. Scientists are now developing new "electronic tattoo BCIs" based on conductive polymer liquid inks that, once dried, form an almost imperceptible thin-film electrode on the skin surface to capture brain activity through the scalp.
3. Semi-Invasive
Semi-invasive BCIs are like observing a planet from satellite orbit. They fall between non-invasive and invasive approaches: electrodes still require surgical placement, but rather than penetrating the cerebral cortex, they adhere like a patch beneath the skull and above the cortex.
Because they avoid skull interference, these BCIs achieve significantly better signal resolution than non-invasive methods. Meanwhile, since electrodes rest above the cortex rather than within it, they face less immune rejection and displacement from brain movement, making them safer than fully invasive approaches. Thus, semi-invasive BCIs are more readily accepted in clinical settings.
In the long term, semi-invasive BCIs may become commercial solutions for paralysis, ALS, and muscular dysfunction; in the near term, they represent important milestones for refining invasive BCI clinical protocols. Hongbo Wang, a professor at Tsinghua University, has collaborated with industry partners to develop a semi-invasive BCI that has completed electrode implantation in three paralyzed patients. On the research front, semi-invasive BCIs have made notable progress in language BCIs and are being explored for visual reconstruction, thought-controlled devices, and other applications.
4. Interventional
Interventional BCIs are like exploring a planet through underground pipelines. They deliver electrodes via intravenous stenting to veins near target brain regions for signal acquisition or modulation.
Benefiting from nearly 50 years of clinical stent use in cardiology, interventional BCIs offer good safety and high stability, with some products already validated through clinical trials. However, blood vessels still substantially shield neural signals, and regions of interest may lack uniform venous distribution. Currently, interventional BCIs can only perform relatively simple tasks, such as cursor control via brain signals.
From a commercialization perspective, interventional BCIs may follow non-invasive BCIs as the next category to reach patients. Synchron, an American company, has developed Stentrode, an interventional BCI implanted subcutaneously and extended via blood vessels to near the motor cortex, where it detects motor cortex electrical signals. Patients can use this device to wirelessly control touchscreens, mice, and keyboards, enabling typing, email, and even opening bank accounts.
II. Based on Interaction Between the Central Nervous System and External Devices
Based on how the central nervous system (CNS) interacts with the BCI, we can classify BCIs into read, write, and read-write fusion types.
Read-type BCIs record brain activity through electrical, magnetic, or blood-oxygen signals, with external devices as the output—such as brain-controlled robotic arms. This is the most common BCI type.
Write-type BCIs input energy or signals into the brain through electrical, magnetic, or ultrasound methods, with external devices as the input—such as visual prosthetics. Since both the target and potential interference source are the brain itself, developing these BCIs requires deep understanding of brain physiology and even higher cognitive processes.
Read-write fusion BCIs integrate both paradigms, enabling coordinated recording and stimulation. These closed-loop BCIs represent the current research frontier, aiming to achieve BCI functions efficiently and in personalized ways.
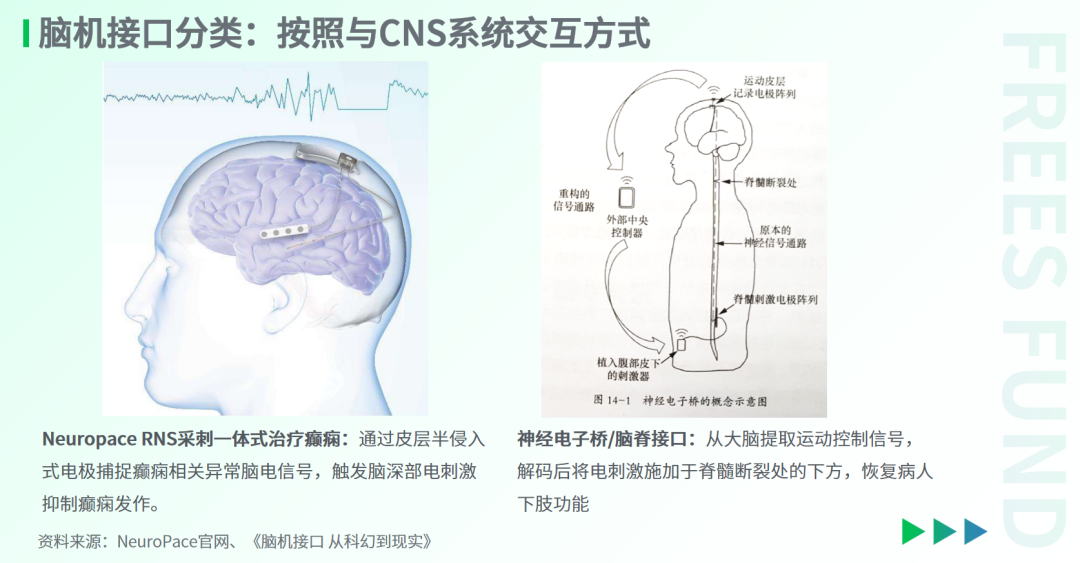
Neuropace's integrated sensing-stimulation implant for epilepsy treatment can be considered the simplest form of read-write fusion BCI. It captures seizure-related abnormal brain signals through semi-invasive cortical electrodes, triggering deep brain stimulation to suppress seizures. Another read-write fusion BCI currently in development is the "neural electronic bridge" or "brain-spine interface," which extracts motor control signals from the brain and applies electrical stimulation below spinal cord injury sites to restore limb function. We will elaborate on this below.
III. By Functional Evolution
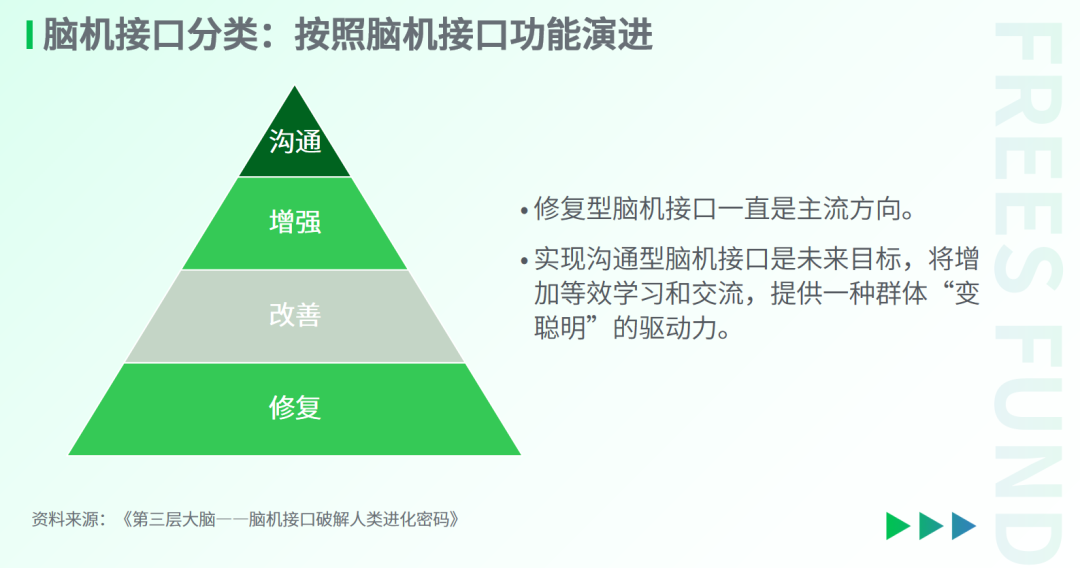
BCIs can be categorized by functional evolution into restorative, augmentative, enhancement, and communication types.
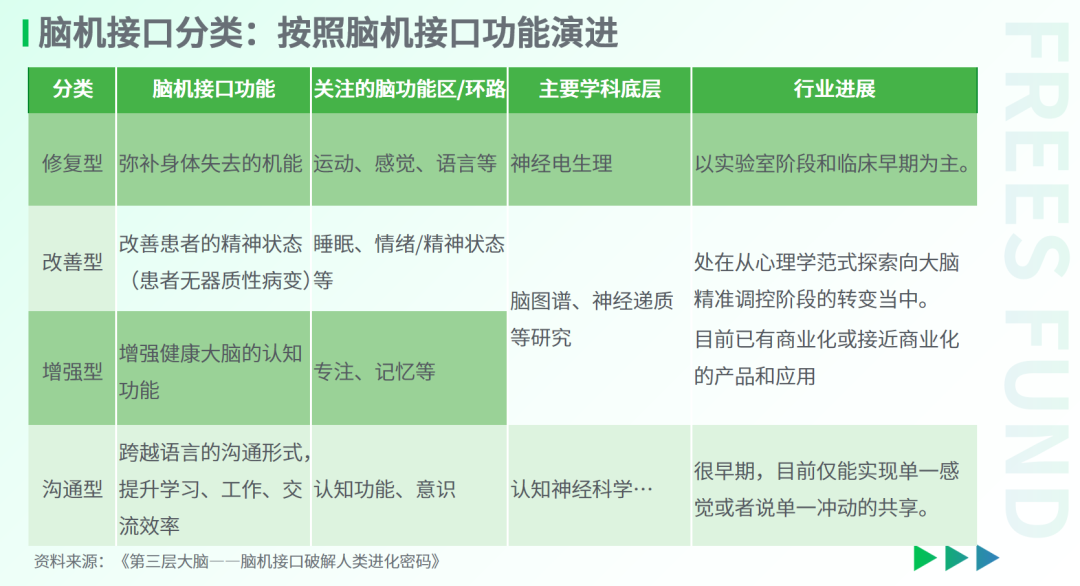
1. Restorative
Restorative BCIs compensate for lost bodily functions, primarily targeting motor (including speech) and sensory systems. The paralyzed former football player who kicked off the World Cup in Brazil, as mentioned in our opening, used a restorative BCI. This category has remained the mainstream research direction. The motor and sensory cortices are relatively large, facilitating neuroelectrophysiological research; moreover, motor and sensory experiments yield the most direct feedback from subjects.
To date, while progress has been made in understanding how the brain encodes movement and sensation, we still cannot establish complete correspondences between human free will and characteristic brain signals. Over half a century of BCI development, restorative BCIs have remained largely in laboratory or clinical trial stages. Future development may require improved decoding capabilities based on more comprehensive data, combined with the brain's own learning processes.
The most successful restorative BCI example is the cochlear implant. According to a BCG report, the global cochlear implant market reached $2.055 billion in 2023. Notably, cochlear implants do not directly stimulate the auditory cortex; instead, different electrodes connect to auditory nerve fibers (spiral ganglion neurons) at different frequencies, mimicking how the cochlea transmits sounds of varying frequencies. Cochlear implants restore the ability to hear different frequencies, not the semantic understanding of sound. After implantation, patients typically need about a year to gradually "comprehend" languages they previously knew, starting from unclear dialogue and indistinguishable sounds.
2. Augmentative
Unlike restorative BCIs, augmentative BCIs are not confined to electrical activity in a single cortical area. They focus on neurotransmitter fluctuations and whole-brain network activity.
The brain is not a passive receiver of objective information. Brain plasticity provides fertile ground for augmentative BCIs, enabling mood regulation and even treatment of mental disorders—such as improving insomnia, managing anxiety, intervening in obsessive-compulsive disorder, and treating depression.
Notably, a paper in Nature Medicine analyzed brain activity patterns across six depression-related networks during resting state and specific tasks in over 800 patients with depression. By quantifying activity levels and connectome patterns in these six network-associated brain regions and comparing them with healthy populations, the authors identified six distinct depression subtypes, each with unique brain activity patterns. Based on these subtypes, the authors applied different treatment strategies to different patients, finding that depression subtypes correlated with different clinical symptoms and treatment responses.
This approach to decoding, subtyping, and treating depression demonstrates that specific brain activity patterns can predict the most effective treatment strategy for individual patients, potentially providing important theoretical support for augmentative BCIs in depression treatment.
3. Enhancement
Augmentative BCIs primarily target patients with psychiatric conditions, while enhancement BCIs aim to boost brain function in healthy individuals — improving focus, strengthening memory, and even enabling multitasking. The development of enhancement BCIs is likewise closely tied to advances in brain mapping research.
One example of an enhancement BCI is the head-mounted brain-computer interface developed by Nissan. In emergency situations, it can transmit brainwave signals to a vehicle to trigger rapid braking. When driving, physical reactions lag behind neural activity; EEG-controlled braking typically saves 0.2 to 0.5 seconds in reaction time. For a car traveling at 120 kilometers per hour, this means initiating braking roughly 7 meters earlier — a significant improvement in driving safety. However, because non-invasive devices record EEG signals with relatively limited precision and real-time performance, and because the human brain typically operates in multitasking mode during driving, the recorded data is complex and highly individualized. The "brain-controlled braking BCI" likely remains years away from practical deployment.
Another already-commercialized example is Feelzing, a BCI product developed by Thync. It uses non-invasive transcutaneous auricular vagus nerve stimulation to enhance focus during task execution. Double-blind controlled trials conducted by the company showed that approximately one-third of participants experienced strong improvements, including heightened mental acuity, better mood and work motivation, reduced mental fatigue, and improved efficiency.
4. Communication
Communication BCIs represent a key focus of future research. Their goal is to enable direct thought exchange that transcends traditional language, thereby accelerating the efficiency of learning, work, and communication — achieving what might be called "tacit understanding" in interpersonal exchange. Communication BCIs will increase the volume of equivalent learning and communicative content, becoming an important driver of progress in "collective intelligence."
In current research, BCIs can only achieve "sharing" of single sensations or single impulses. In 2018, the University of Washington conducted an experiment in which three people collaborated to play Tetris. By extracting EEG signal features from the visual cortex and transmitting "impulse" sensations via transcranial magnetic stimulation, the experiment preliminarily verified that humans can coordinate on tasks through EEG signals alone, without verbal communication.
04 The Neuroscientific Principle of BCIs: Proprioception
In our previous brain science research, we mentioned certain principles such as neuroplasticity — the capacity of neurons to regenerate and form new connections. These newly formed connections can enable certain brain regions to function in ways different from before.
In this article, we will examine in detail another, less frequently discussed principle: proprioception, which we can consider an extension of neuroplasticity.
The brain is not merely an information receiver; it can also reconstruct the external world, incorporating external objects into its self-perception. This extended cognitive capacity is known as "proprioception" or "peripersonal space."
What we normally perceive is more of a "map" transmitted by the brain — not necessarily the true state of the body. Our peripersonal space is built upon our body schema and tools. This peripersonal space can even encompass virtual worlds within computers.
For example, when holding a tool, our bodily perception can extend to the tool's tip, as if the tool were part of our body. Another vivid example is "road feel" — the holistic sense of vehicle and driver movement that people develop while driving, where perception expands from the individual to the various vertices and contours of the car.
BCIs likewise establish a kind of "interface feel" in patients. Based on the brain's capacity to be shaped, the brain "adapts" to the device, eventually perceiving it as part of the self.
Experiments at University College London further validated this phenomenon: when participants used a foot-controlled robotic finger as a "sixth finger" to complete tasks, the brain gradually adapted to the robotic finger's presence, perceiving it as a normal extension of the body. Subjects could easily coordinate the five fingers of one hand with the foot-controlled sixth finger, performing actions such as solving math problems while building with blocks, or making various gestures while blindfolded.
▲ Participants used a foot-controlled robotic finger as a "sixth finger." Image source: University College London robotic finger experiment.
Later, brain imaging results showed that after training, the brain activity patterns corresponding to each finger became more similar, and the motor signals of toes and fingers also grew more alike. This remodeling persisted for 7 to 10 days after training ended. This adaptive change in brain activity patterns provides scientific grounding for BCI devices being "accepted" by humans as part of the body.
The human brain adapts to tools that extend peripersonal space as if they were part of the body. Similarly, ideal BCIs that help humans expand their peripersonal space will ultimately be adapted to by the body.
05
The Development Trajectory of BCIs: From Science Fiction to Reality, From Research to Technology to Clinical Application
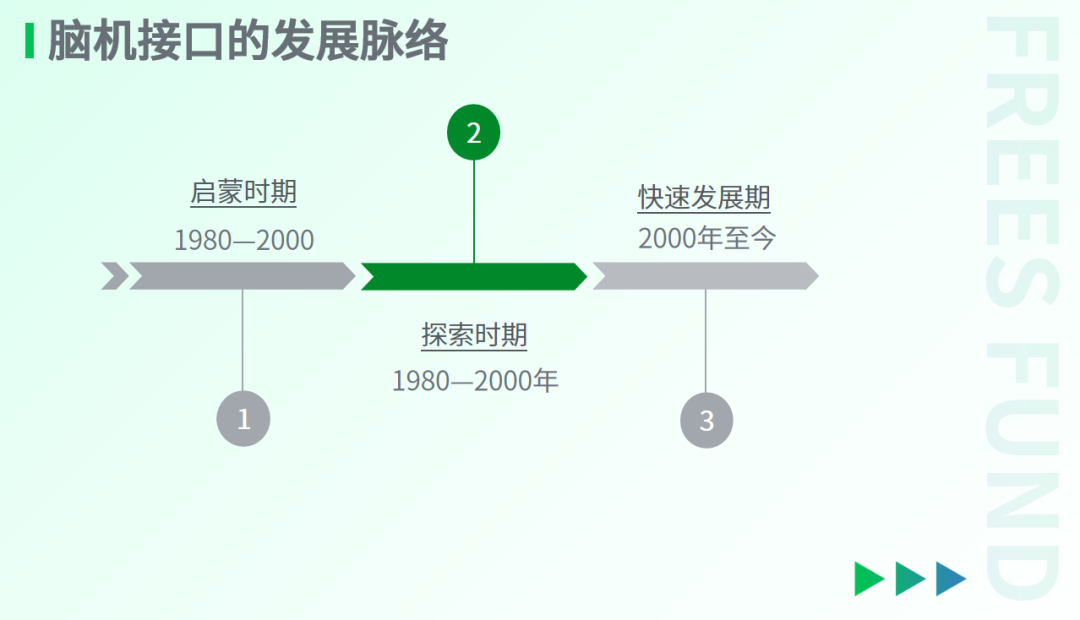
I. The Enlightenment Period (Before 1980)
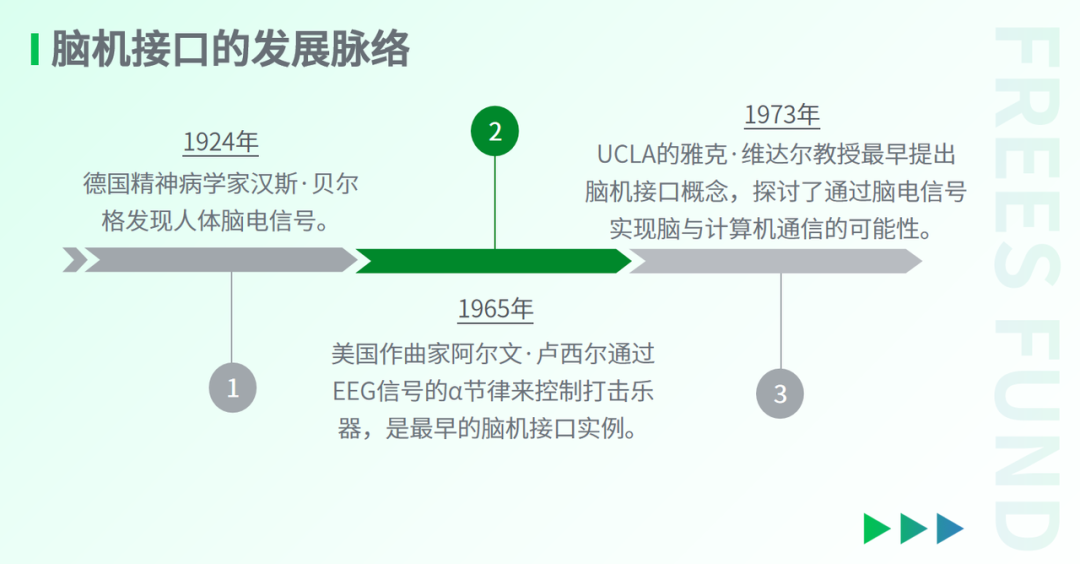
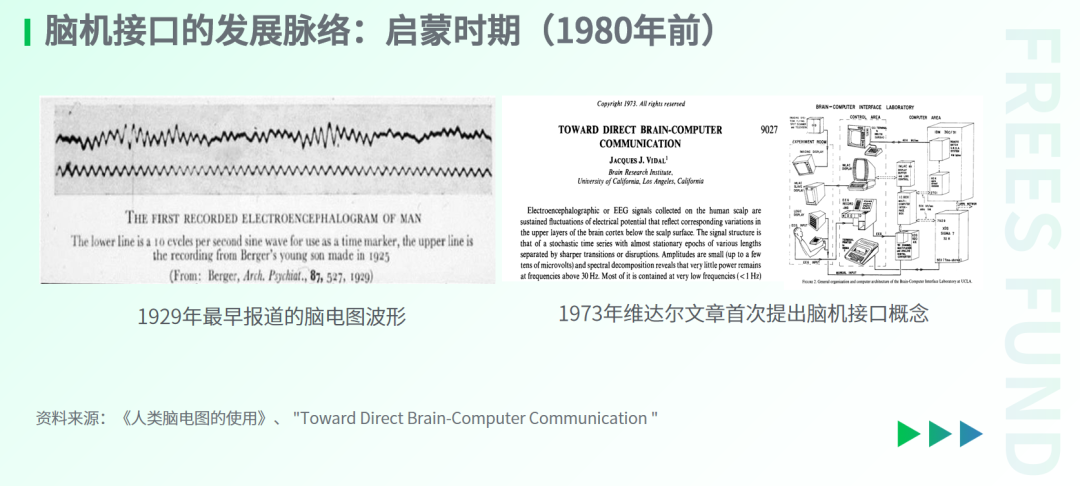
The history of BCIs can be traced back to the discovery of brain electricity. In 1924, German psychiatrist Hans Berger recorded tiny oscillations in a galvanometer mirror near the scar on a 17-year-old boy's head. This was the first recording of human brain electrical activity in history.
This electrical signal produced by the human brain — what we now know as the EEG (electroencephalogram) signal — is a representation of cortical neuronal electrical activity.
Berger further discovered that different brain states produce different EEG characteristics. For example, when a person is awake and relaxed, the brain exhibits alpha waves at 8–13 Hz, while during logical thinking activities, it exhibits beta waves at 13–30 Hz.
In 1965, American composer Alvin Lucier captured the rhythmic signals of his own alpha waves to control the rhythm of percussion instruments, completing a unique performance. This was the first instance of humans achieving direct interaction with external devices through EEG signals, arguably the earliest example of a brain-computer interface.
The discovery of brain electricity and research in neuroelectrophysiology laid crucial foundations for the emergence of BCIs. Additionally, between 1950 and 1970, the advent of integrated circuits, the invention of digital computers, and signal processing performed by computers provided the technical means for in-depth analysis of continuously varying EEG signals.
When these elements "came together" around 1970, the concept of the brain-computer interface was born. In 1973, Professor Jacques Vidal at UCLA first proposed the concept of the brain-computer interface, beginning to explore how EEG signals could enable direct brain-computer communication.
Overall, the discovery and interpretation of EEG signals established the main direction of BCI development. Although functional magnetic resonance imaging, magnetoencephalography, and functional near-infrared spectroscopy can also record brain activity and even perform certain decoding, EEG signals remain the primary source of brain information for BCIs.
II. The Exploration Period (1980–2000)
1. Non-Invasive BCI Research Phase
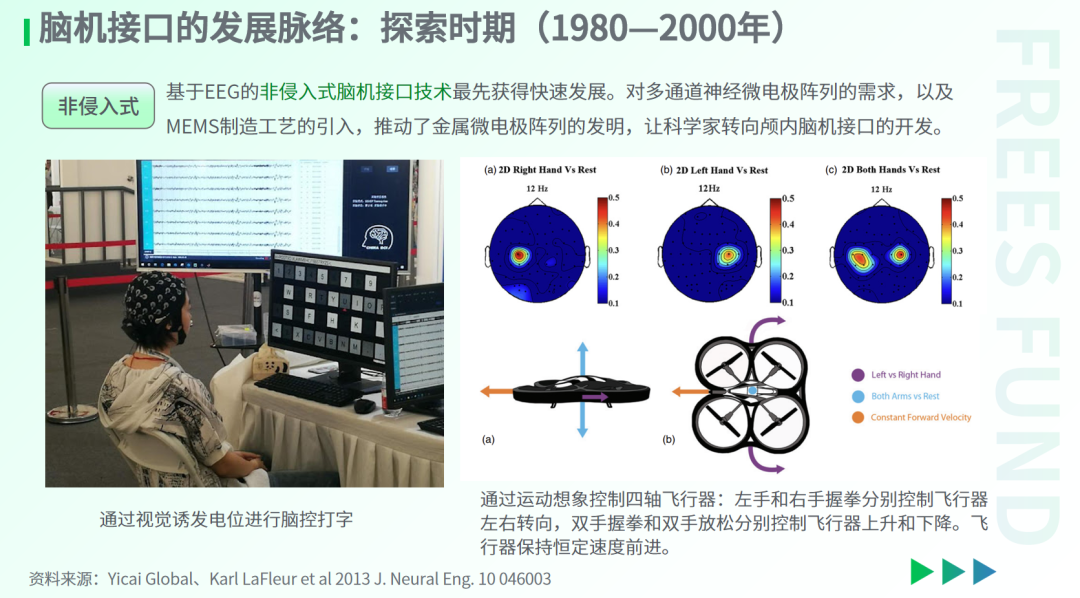
From the 1980s to 2000, BCI research entered a phase of deep exploration. On one hand, scientists built upon early non-invasive EEG signal studies to make initial attempts at BCIs, achieving progress in interfaces based on visual evoked potentials and hand motor imagery signals.
Visual evoked potentials are recorded by measuring the brain's response to visual stimuli at specific frequencies. When subjects see icons flickering on screen at particular frequencies — even frequencies beyond the range of conscious visual discrimination — the brain can still effectively "capture" these signal frequencies and manifest them in the EEG. By designing specific visual input frequencies, external devices can be controlled indirectly, such as typing via a soft keyboard.
Hand motor imagery involves controlling external devices by imagining specific hand gestures. The hand was chosen because the cortical areas associated with hand motor imagery occupy a large proportion of the motor and sensory cortex; motor imagery of the hand readily produces characteristic signals detectable by EEG.
Notably, Professor Xiaorong Gao of Tsinghua University developed a visual evoked potential-based BCI in 2002, with which subjects could dial a pager by looking at numbers on a screen — leading globally at that time.
This research paradigm of non-invasive BCI technology for spelling control, wheelchair control, and simple communication has persisted to this day.
However, EEG signals have certain limitations. Since EEG only records horizontal potential differences at the scalp surface, it cannot capture vertical electrical activity deep in the cerebral cortex — and vertical currents typically carry relatively rich cognitive and motor information. Thus, the information conveyed by EEG signals is somewhat limited. More importantly, EEG cannot be directly and simply correlated with an individual's free will; it generally relies on external stimuli to elicit cortical responses and identify characteristic EEG signals for indirect control of external devices, greatly limiting its scope of application.
Therefore, during the same period, scientists were also developing electrodes for invasive BCIs that penetrate into the brain.
2. Invasive BCI Research Phase
The earliest type of invasive BCI was the neurotrophic electrode invented by Phil Kennedy at the Georgia Institute of Technology, designed to record changes in electrode signals. He ingeniously incorporated peripheral nerve fragments such as the sciatic nerve into the electrode. Experiments demonstrated that after implantation in the brain, these fragments were accepted by surrounding neurons, which helped reduce immune rejection responses. Additionally, the neurotrophic electrode used a glass cone to create an insulating barrier around the electrode and the ingrowing neural axons, amplifying extracellular action potentials.
In 1998, scientists conducted the first clinical trial of an invasive motor BCI. Two neurotrophic electrodes were implanted in a patient's primary motor cortex, enabling the patient to control cursor movement and typing through imagined hand movements. Even six months after implantation, the patient maintained relatively high typing speed and accuracy.
The implantation sites for neurotrophic electrodes were limited. To capture neural activity across a broader swath of the cerebral cortex, the Michigan electrode and the Utah electrode emerged during this period. The Michigan electrode used micro-nanofabrication techniques to create one-dimensional and two-dimensional electrodes on silicon wafers, capable of collecting neural signals across a larger area. This fabrication approach solved problems of inconsistent electrode sizing and positional variation that plagued traditional manual assembly, substantially improving experimental reproducibility.
The Utah electrode was another invasive BCI electrode based on micro-nanofabrication. Compared to the Michigan electrode, its unique structural design and material improvements delivered more stable electrical performance and mechanical structure. In the early 2000s, the Utah electrode obtained FDA approval for clinical trials ahead of the Michigan electrode, becoming one of the clinical standards for BCI electrodes.

3. Rapid Development Period (2000–Present)
Since the turn of the 21st century, clinical research on invasive BCIs has accelerated significantly following FDA approval of the Utah electrode for clinical trials. In 2002, Professor John Donoghue at Brown University developed a BCI device that helped a stroke patient successfully pick up a water cup using a robotic arm controlled by thought.
Invasive BCIs have also made notable progress in language restoration. In 2021, a team led by Professor Krishna Shenoy at Stanford University implanted Utah electrodes in the motor cortex of a patient with arm paralysis, capturing the patient's intention signals for handwriting letters and converting them into text. Through sophisticated neural network algorithms, the patient achieved a writing speed of 90 letters per minute with over 90% accuracy.
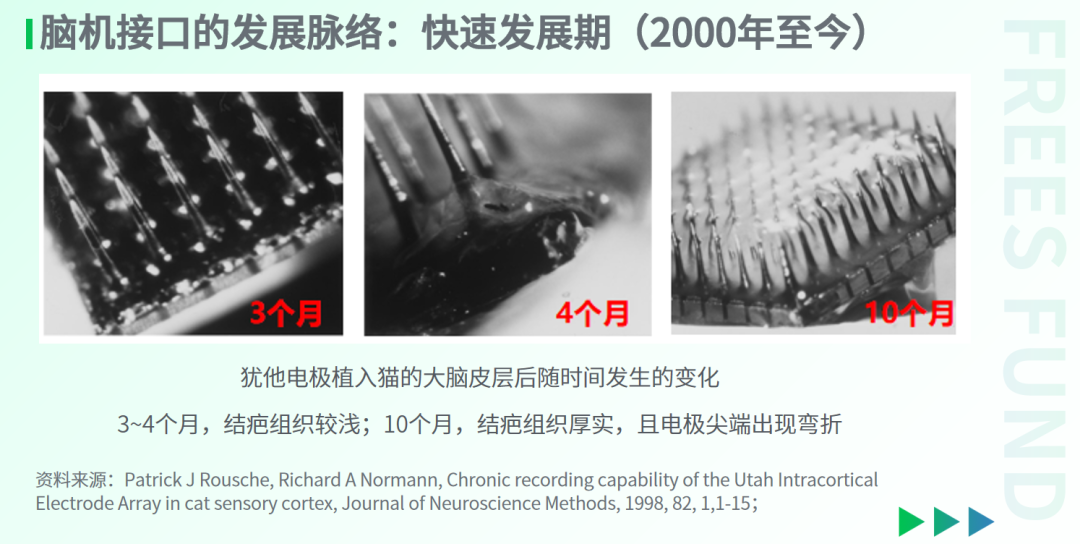
However, alongside these initial functional validations of the Utah electrode in clinical settings, researchers discovered that long-term implantation caused severe immune rejection, gradually degrading the electrode's ability to record electrical signals while potentially compromising brain health. One surprising experimental finding: when Utah electrodes were implanted in a cat's cerebral cortex, over time they became encased in thick, dense scar tissue, and in some cases the rigid electrode tips were actually "bent" by the brain tissue itself.
Meanwhile, invasive electrodes faced another challenge: the brain's rhythmic pulsation with each heartbeat caused traditional rigid electrodes to remain unstable around specific neurons, with continuous displacement compromising recording stability.
These problems of immune rejection and positional uncertainty drove researchers to develop new electrode materials and designs. To date, three approaches have emerged: flexible electrodes, semi-invasive electrodes, and interventional electrodes.
As mentioned earlier, semi-invasive and interventional electrodes significantly reduce immune rejection, but they are weaker than invasive electrodes in precision and the amount of electrical signal information recorded.
Flexible electrodes, which must penetrate the brain, employ tiny mesh or thread-like structures with high toughness — their material is even softer than neurons themselves. In theory, flexible electrodes can match neuronal dimensions and wrap around their surfaces, enabling high-quality recording of neuronal electrical activity while reducing physical damage to the brain. On the other hand, development of flexible electrodes for BCIs has already exceeded ten years, with materials, electrode fabrication processes, and surgical implantation protocols still being widely explored in both research and industry. The immune response and long-term implantation safety of flexible electrodes remain to be validated over extended periods.
06
Breakthrough and Balance: Reflections on BCI Commercialization
Today, BCI companies are entering the commercialization phase. In the flexible electrode space, for example, Neuralink — co-founded by Elon Musk — has developed a BCI using microwire electrodes and obtained FDA approval for clinical trials.
As a frontier technology spanning neuroscience, computer science, and engineering, BCI demonstrates tremendous potential. Yet its path to commercialization requires breakthroughs and balance across multiple dimensions: benefits, risks, ease of use, and market accessibility.
Invasive and non-invasive BCIs face somewhat different commercialization challenges.
Safety represents the primary challenge for invasive BCIs, encompassing trauma from craniotomy surgery, immune rejection reactions triggered by electrode materials, and potential risks from long-term brain implants. These safety concerns not only affect acceptance among patients and clinicians but also create hurdles during the regulatory approval process.
Non-invasive devices offer high safety, but most current devices lack sufficient comfort for everyday use. Therefore, achieving lightweight, portable designs comfortable enough for extended wear represents a critical development direction for non-invasive BCIs.
Matching differentiated technical approaches with precisely targeted application scenarios is key to commercialization.
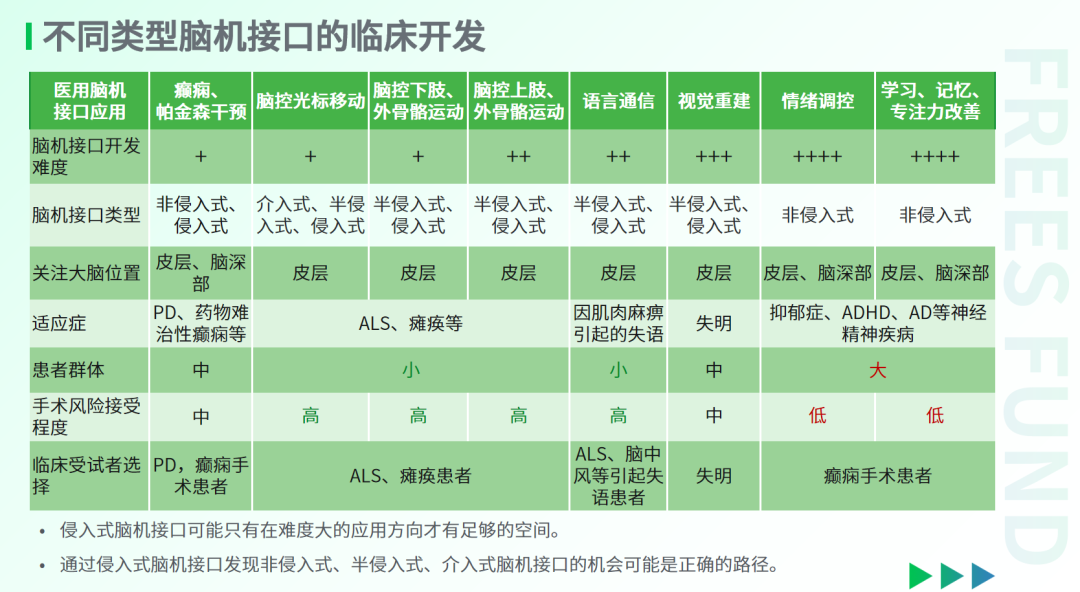
Invasive BCIs primarily address refractory or terminal conditions such as drug-resistant epilepsy, ALS, and complete paralysis. Given the severity of these diseases, patients demonstrate higher acceptance of surgical risks, constituting the potential market for invasive BCIs. The main applications focus on restoring or replacing motor function, including brain-controlled cursor movement, brain-controlled exoskeleton locomotion, and brain-controlled language communication. However, the relatively small patient population limits commercialization potential.
Applications targeting mental health intervention, emotional regulation, and learning and memory enhancement typically address much larger user populations, but these users show relatively lower acceptance of surgical risks. Therefore, over the long term, non-invasive BCIs are better suited to these application scenarios.
For visual restoration, the patient population is substantial, and compared to the quality-of-life degradation caused by blindness, patients are likely to accept the risks of BCI implantation surgery. Thus, visual restoration may become a promising commercialization direction for semi-invasive and invasive BCIs.
From the perspective of BCI development pathways, commercialization will require multiple technical approaches. Non-invasive, semi-invasive, and interventional BCIs currently lead invasive BCIs in clinical development progress, but their functional iteration will increasingly depend on "in-situ" brain electrical data recorded by invasive BCIs. Specifically, invasive therapeutic devices for refractory epilepsy, Parkinson's disease, and other brain disorders, along with invasive BCIs gradually entering clinical use for serious conditions such as ALS and complete paralysis, will over the medium to long term provide the data foundation for developing non-invasive and semi-invasive BCIs capable of complex tasks — forming a technology-gradation commercialization pathway.
**/ 07 / **
What Future BCIs Can We Imagine?
The future applications of BCI are vast. From vision to emotion to memory, BCI technology will extend far beyond restoring motor and language function to comprehensively enhance human quality of life and cognitive capabilities.
1. Brain-Spine Interface
The brain-spine interface, also known as a "neuroelectronic bridge," aims to extract motor control signals from the brain and apply electrical stimulation below the site of spinal cord injury to restore limb function in patients.
A key assumption underlying the brain-spine interface is that control of lower limb movement patterns is executed by neural circuits within the lumbar spinal cord, while the brain and cerebellum merely issue signals to initiate, terminate, and modulate movement. For example, the initiation, termination, distance, and speed of walking are determined by the cerebrum and cerebellum, while the continuous control algorithm for locomotion is "stored" in the lumbar region. Therefore, the core of the brain-spine interface lies in understanding the intentions of the cerebrum and cerebellum and activating corresponding movement patterns in the lumbar cord — establishing the mapping from "brain motor intention → electrical stimulation sequence pattern on the dorsal spinal cord → target electrical activity pattern sequence in spinal motor neurons."
In 2021, scientists used a brain-spine interface to help a paralyzed monkey walk again. Through continued research and refinement, this technology may become an important means of restoring motor function in spinal cord injury patients.
▲ A brain-spine interface helped a paralyzed monkey walk again
Video source: A brain–spine interface alleviating gait deficits after spinal cord injury in primates, Nature, 2016, 539, 284
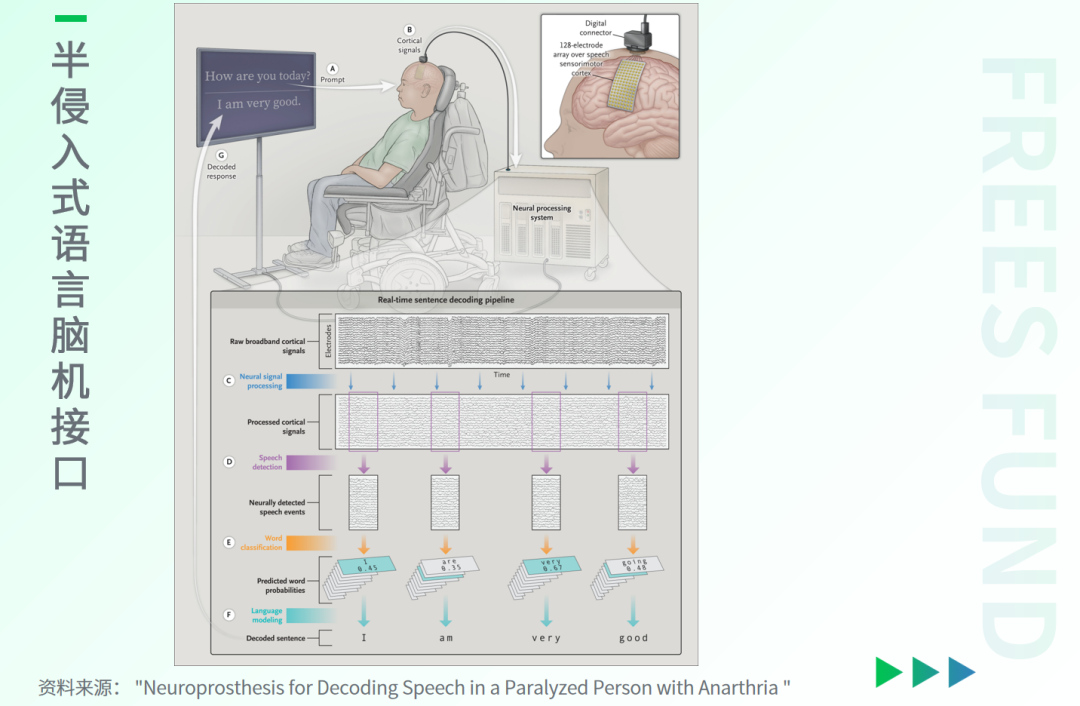
2. Semi-Invasive Language BCI
Language BCIs are communication tools designed for paralyzed patients who cannot speak. Conditions such as brainstem stroke, traumatic brain injury, and ALS can damage patients' motor neurons, robbing them of the ability to express themselves verbally. Though these patients remain fully conscious and cognitively intact, they cannot communicate through speech or gesture. Semi-invasive language BCIs address this by placing electrode arrays on the patient's cerebral cortex to capture intention signals and convert them into text or speech, helping patients express their needs once more.
3. Sensory and Cognitive Enhancement BCIs
- Visual BCI: Three retinal prostheses have currently received FDA approval, capable of partially restoring vision in visually impaired individuals. However, because surgery and stimulation in the eye present significant difficulties, these products have all been discontinued. Direct implantation of BCIs in the visual cortex to help patients with acquired blindness regain visual experience may be the only viable approach. The core challenges lie in combining basic visual information such as brightness, orientation, color, motion, and depth, and in determining how to write this information into the human brain.
- Emotion-Regulating BCI: Detecting and modulating neurotransmitter levels in the brain to intervene in patients' mental and emotional states, which holds major significance for treating severe psychiatric conditions.
- Somatosensory BCI: Providing realistic tactile feedback for artificial limbs, enabling users to better control prosthetics.
- Memory BCI: Enhancing long-term memory by strengthening or modulating synchronized activity across multiple brain regions.
**/ 08 / **
How to Invest in BCIs?
Overall, the market potential for brain-computer interfaces is vast. Whether non-invasive, invasive, semi-invasive, or interventional BCIs, each has suitable application scenarios at different stages of industry development. Clinical validation represents the first milestone on the path to commercialization, and clinical deployment requires balancing patient risk against benefit while prioritizing ease of use.
I. Non-invasive BCIs have seen numerous commercial attempts
The non-invasive BCI direction has already generated considerable experimentation in research, clinical, and commercial settings due to its relatively low safety risks.
On the "reading brain" side, signal resolution limitations mean diminishing marginal returns for EEG-based product development. Consequently, multimodal brain imaging that integrates structural, blood-oxygen, and magnetoencephalography signals has become a research hotspot in scientific and clinical contexts.
On the commercial side, companies will particularly focus on improving product convenience and promoting consumer-oriented applications.
On the "writing brain" side, transcranial electrical stimulation, transcranial magnetic stimulation, temporal interference stimulation, and transcranial ultrasound stimulation offer novel approaches to understanding brain function by modulating neural activity at mesoscopic to macroscopic scales. Personalized, closed-loop neuromodulation based on neuroimaging may represent the next frontier. Non-invasive neuromodulation will also provide greater "preclinical support" for the development of invasive BCI applications.
II. Semi-invasive and interventional BCIs are approaching an inflection point for productization and commercialization
In medical scenarios for patients with paralysis, speech loss, or disability, semi-invasive and interventional approaches have produced fully integrated, implementable solutions for brain-controlled computer interaction, language communication BCIs, and motor rehabilitation via brain-spine interfaces. This class of medical BCIs is expected to balance the need for micro- to mesoscopic-scale neural signal acquisition with clinical acceptability, gradually reaching an inflection point for productization and commercialization.
III. Invasive BCIs remain in the early stages of industry development
Invasive BCI development requires sustained R&D and long-term validation, and the field remains in its early stages. Microelectrodes or microelectrode arrays constitute the core of current invasive BCI development. Microelectrodes provide the only clinically available observation method spanning microscopic (single neuron) to mesoscopic (projected million-neuron scale) resolution. Advances in electrode development, along with innovations in neural decoding algorithms and electrical stimulation paradigms, will inevitably drive clinical progress.
The focus of invasive BCI development will gradually shift from electrodes toward applications. On one hand, long-cycle validation remains pending for immune rejection of flexible materials in invasive electrodes and extended human use (for instance, the FDA requires permanently implanted medical devices to remain safe in vivo for at least ten years); during this phase, primary value creation will migrate toward the application side. On the other hand, developing applications beyond motor systems — such as sensory restoration, emotional regulation, and higher cognition — involves substantial expertise barriers in neuroscience and algorithms, making clinical deployment potentially more valuable.
Therefore, we believe that from the perspectives of both clinical acceptance and commercial value, non-invasive, semi-invasive, and interventional BCIs will outpace invasive BCIs in the near term. As the value of more precise "in-situ" neural data gradually becomes apparent and clinical risks are progressively mitigated, invasive BCIs will become an essential technical pathway in the medium term. Looking further ahead, invasive BCIs will also drive the development of semi-invasive and even non-invasive BCIs capable of executing more complex tasks. Value growth in the first half lies in the accumulation of human brain data; the core value in the second half lies in application scale.
Brain-computer interfaces are no longer science fiction or mere concept — they have become a tangible, investable domain. For investment decision-making in BCIs, one approach is to comprehensively evaluate the maturity of differentiated technical pathways, the risk-benefit profile of deployment scenarios, and the commercial value potential of applications; another is to think backward from the end state, identifying critical milestones along the path and focusing on value growth in vertical domains.
| References
[1] Guo Liang (U.S.). Brain-Computer Interfaces: From Science Fiction to Reality [M]. Beijing: Posts & Telecom Press, 2024.
[2] Sun Yu. The Third Brain: How Brain-Computer Interfaces Crack the Code of Human Evolution [M]. Beijing: Publishing House of Electronics Industry, 2022.
[3] A brain–spine interface alleviating gait deficits after spinal cord injury in primates, Nature, 2016, 539, 284.
[4] Francis R. Willett et al., High-performance brain-to-text communication via handwriting, Nature, 593, 249-254.
[5] Henri Lorach et al., Walking naturally after spinal cord injury using a brain–spine interface, Nature, 2023, 618, 126-133
Jacques J Vidal, Toward Direct Brain-Computer Communication, Annu. Rev. Biophys. 1973, 2, 157-180.
[6] Leigh R. Hochberg et al., Reach and grasp by people with tetraplegia using a neurally controlled robotic arm, Nature, 2012, 485, 372-375.
[7] Luize Scalco de Vasconcelos et al., On-scalp printing of personalized electroencephalography e-tattoos, 2024. DOI: 10.1016/j.celbio.2024.100004
[8] Ming Cheng et al., Design and implementation of a brain-computer interface with high transfer rates, IEEE Transactions on Biomedical Engineering, 2002, 49, 10, 1181-1186.
[9] Paulina Kieliba et al., Robotic hand augmentation drives changes in neural body representation, Sci. Robot., 2021, 6, eabd7935.
[10] Sean L. Metzger et al., A high-performance neuroprosthesis for speech decoding and avatar control, Nature, 2023, 620, 1037-1046.
[11] Suseendrakumar Duraivel et al., High-resolution neural recordings improve the accuracy of speech decoding. Nat. Commun. 2023, 14, 6938.
[12] Antoine Remy et al., Materials for flexible and soft brain‑computer interfaces, a review, MRS Communications, 2024, 14, 827-834.
What changes do you hope BCI technology will bring to everyday life? Leave a comment below — we'll randomly select five readers to each receive a copy of Brain-Computer Interfaces: From Science Fiction to Reality.

▲ Biomanufacturing: Who Can Move Faster Under the New Research Paradigm?
▲ Outlook 2025: What Innovation Opportunities Await the AI Industry? | FreeS Report
▲ LiDAR or Cameras? How We View the Autonomous Driving Route Debate
▲ FreeS Report 24 | Embracing the "Smartest" Windfall: Investing Boldly in Brain and Neuroscience
▲ The Human Body's "Smartest" Organ: How Can We Explore It Further? | FreeS Research
Star the FreeS Fund WeChat official account for timely business insights delivered to your feed