Everything Has Two Sides: How Can "Nuclear Radiation" Be Used to Make Anti-Cancer Drugs? | FreeS Report 28

Now is the spring of radiopharmaceuticals.
Today's report focuses on nuclear medicine — drugs associated with nuclear medicine, also known as radiation medicine. The "nuclear" in "nuclear medicine" doesn't refer to nucleic acids, but rather to the "nuclear" in nuclear radiation, which can sound frightening at first. Yet everything has two sides, and nuclear technology can also bring hope to people suffering from cancer.
In 2018, Lutathera (lutetium Lu 177 dotatate), a nuclear medicine developed by a Novartis subsidiary, received FDA approval for treating pancreatic neuroendocrine tumors. Apple founder Steve Jobs died from a pancreatic tumor. Beyond pancreatic tumors, nuclear medicine can also treat prostate cancer, meningioma, thyroid cancer, lymphoma, and other malignancies.
If we were to crown one discipline the "king of interdisciplinary fields," radiation medicine might well take first place — with no close second. Radiation medicine is an emerging discipline that uses nuclear technology to diagnose, treat, and research diseases. It encompasses molecular imaging (PET-CT, diagnostic radiopharmaceuticals), external beam radiotherapy (proton and heavy ion therapy), and internal radiotherapy (therapeutic radiopharmaceuticals). It draws on knowledge from physics, chemistry, biology, medicine, computer science, and more — a product of modern science and technology converging with medicine.
In recent years, nuclear medicine has gradually demonstrated its potential in cancer treatment and brain disease diagnosis and treatment. It shows unique advantages in precision quantitative dosing, combining internal and external radiation, and integrating diagnosis with therapy — capabilities that traditional drugs struggle to match. This report focuses primarily on therapeutic radiopharmaceuticals, while also covering some aspects of molecular imaging and external beam radiotherapy.
We will also discuss nuclear medicine in the context of China's major push to develop nuclear energy. China has surpassed France to become the world's second-largest producer of nuclear power after the United States. In terms of nuclear power plants under construction, China has ranked first globally for 16 consecutive years. The government has introduced numerous policies favorable to nuclear medicine development and is investing in the nuclear medicine supply chain.
In this article, you will learn:
- Is nuclear radiation really as scary as we think, or is it all about dosage?
- Why is now a good time to develop nuclear medicine?
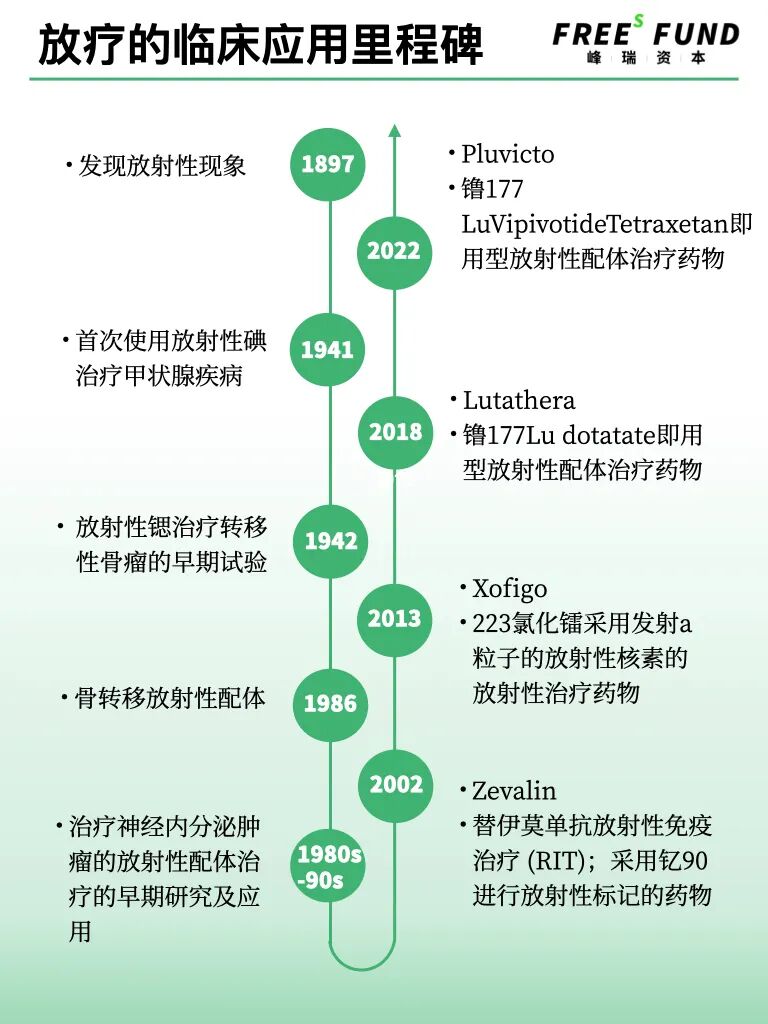
- How did nuclear medicine evolve from humanity's first discovery of radioactivity in 1897 to today?
- Why hasn't nuclear medicine developed faster before now?
- What advantages does nuclear medicine offer in cancer treatment?
- What is the key to nuclear medicine design?
- How does nuclear medicine enable quantitative dosing?
- How does nuclear medicine integrate diagnosis and treatment?
Perhaps right now is the springtime for nuclear medicine's growth.

Since its founding, FreeS Fund has consistently focused on uncovering projects with distinctive interdisciplinary characteristics. We look forward to meeting more entrepreneurs in the nuclear medicine field. Please feel free to contact the author of this article, Shen Jiong, Managing Partner at FreeS Fund (shenjiong@freesvc.com).
Engagement Giveaway
What changes do you think nuclear technology has brought to our lives? Share your thoughts in the comments. The 5 most thoughtful commenters will each receive a copy of Life Atomic: A History of Radioisotopes in Science and Medicine. This book details how nuclear energy was applied to science and medicine after World War II. We look forward to your contributions.


/ 01 /
"Fear of Nuclear": Don't Talk About Toxicity Without Talking About Dosage
Mention "nuclear" or "radiation," and many people immediately think of harm to the body — nuclear weapons, the Hiroshima atomic bombing, the Chernobyl disaster, the Fukushima nuclear leak... But radiation is actually unavoidable in daily life. Talking about toxicity without considering dosage doesn't mean much.
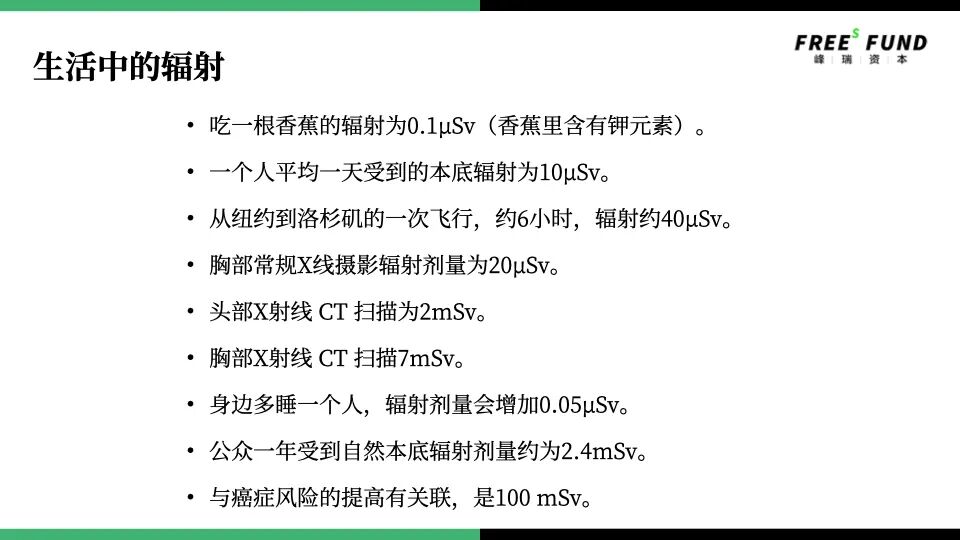
Many foods contain naturally occurring radioactive substances, but in such minuscule amounts that they are essentially harmless to humans. The unit commonly used to measure radiation dose is the sievert (Sv), which represents the total harm from radiation exposure to an individual.
Eating bananas (which contain radioactive potassium), flying on airplanes, getting CT scans — all of these expose you to radiation. Even sleeping next to another person increases your radiation dose by 0.05 μSv.
According to standards set by the International Atomic Energy Agency and China's Basic Standards for Protection against Ionizing Radiation and for the Safety of Radiation Sources, the public exposure limit is 1 mSv per year, and 50 mSv for a single tissue or organ.
You'd need to fly more than 500 times in a year to exceed safety limits. In daily life, though, frequent X-rays and CT scans can easily push you over the limit.
Among radiation dose units, radioactivity intensity and exposure are physical concepts, while equivalent dose and effective dose are biological and medical concepts. Let's focus on equivalent dose and effective dose.
Equivalent dose: Used to express the different biological effects produced by different types and energies of radiation. Its unit is the sievert (Sv), often expressed as mSv, μSv, or nSv in practice.
Effective dose: Used to express the varying sensitivity of different human tissues or organs to radioactive exposure. This unit accounts for both the type of radiation and tissue weighting factors. Its specialized name is also the sievert (Sv).
With these radiation dose units clarified, let's examine what impact nuclear accidents actually have — using a precise, quantitative perspective.
Epidemiological studies of populations exposed to radiation (such as atomic bomb survivors or patients receiving radiotherapy) show that doses exceeding 100 mSv significantly increase cancer risk. For children, even lower doses (50–100 mSv) may elevate cancer risk.
Scientists at the Norwegian Institute for Air Research investigated the Fukushima nuclear accident's radiation leak and found that direct radiation exposure was relatively low. Most people globally received about 0.1 mSv, Japanese people received 0.5 mSv, and Fukushima-area residents received up to 1–5 mSv in the three months following the accident. While 1–5 mSv falls within safety limits, this doesn't mean radioactive water can be casually dumped into the ocean.
In 1986, the Chernobyl disaster occurred in the former Soviet Union. According to Russian estimates, cleanup workers received very high radiation doses, ranging from 10 mSv to 1 Sv, averaging 120 mSv. Eighty-five percent of personnel had internal radioactive doses between 20–500 mSv. These figures show Chernobyl's substantial bodily impact.
In March 2023, a study published in Science Advances examined 302 stray dogs living near the Chernobyl nuclear plant. Theoretically, these dogs shouldn't have survived strong radiation. Yet over three decades, they not only survived but bred for 15 generations. How nuclear radiation affected their DNA mutations and heredity remains a fascinating research question.
/ 02 / Why Is Now the Right Time for Nuclear Medicine?
China's nuclear medicine sector is heating up. China Isotope & Radiation Corporation (under CNNC) and private company Dongcheng Pharmaceutical had already established positions in nuclear medicine, becoming the two dominant players.
In September 2022, Simcere Pharmaceutical's lutetium Lu 177 dotatate injection completed enrollment of its first Phase III clinical trial subject.
In January 2023, Hengrui Medicine's lutetium Lu 177 dotatate injection received clinical trial approval.
In February 2023, Grand Pharmaceutical Group's globally innovative radionuclide drug conjugate TLX101 had its China IND application accepted. Additionally, numerous startups have entered the nuclear medicine race.
The government has introduced many policies favorable to nuclear medicine development. In 2021, the China Atomic Energy Authority, Ministry of Science and Technology, Ministry of Public Security, and five other ministries released the Medium- and Long-Term Development Plan for Medical Isotopes (2021–2035). In 2022, the Center for Drug Evaluation of the National Medical Products Administration issued the revised Administrative Measures for Radioactive Drugs.
The government is also investing in the nuclear medicine supply chain. At the end of 2022, CNNC Qinshan launched construction of China's largest medical isotope production base. CGN also built a medium-energy cyclotron (a particle accelerator for producing medical isotopes) in Mianyang, Sichuan.
Zooming out, the development of nuclear medicine rests on China's long-term investment and construction in nuclear energy.
When we discuss new energy, we typically focus on wind, solar, and hydro. According to IAEA data, China became the world's second-largest nuclear power producer after the US in 2020, and retained that position in 2021.
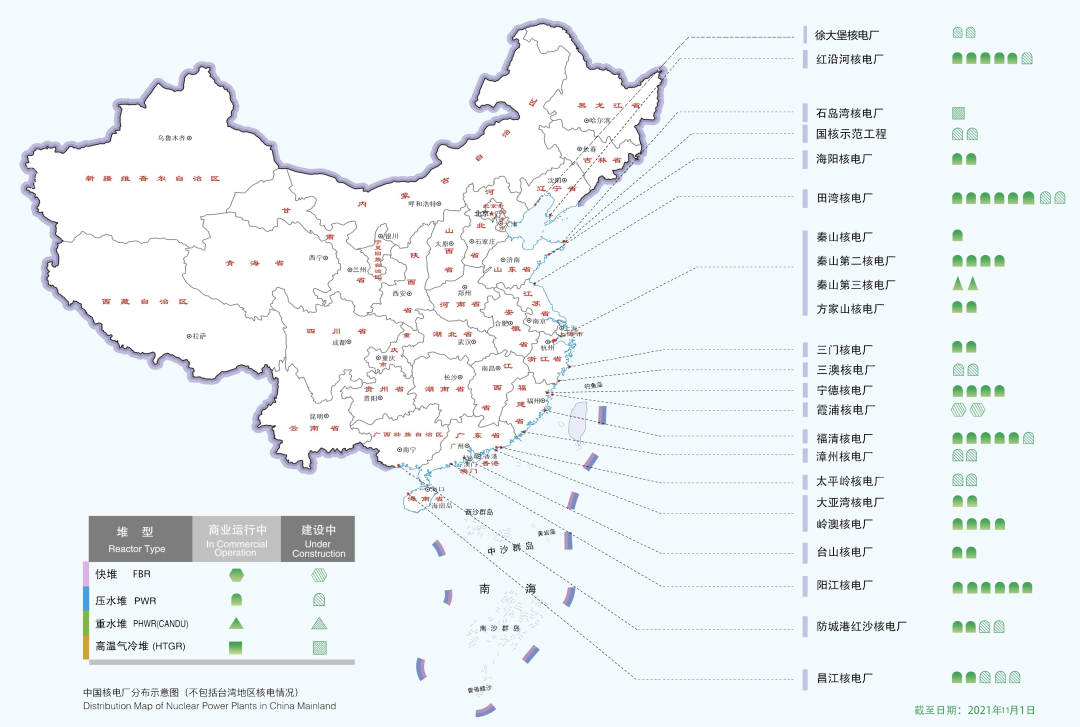
▲ China has the most nuclear power units under construction in the world. According to data disclosed by the China Institute of Nuclear Industry Strategy, as of the end of 2022, mainland China had ranked first globally in nuclear power units under construction for 16 consecutive years.
Because nuclear power plants require water for cooling, they must be built in coastal areas. And China's coastal regions are economically developed with high electricity demand. Multiple factors have converged, leading China to build a large number of nuclear power plants along its coast.
In our view, there are two main reasons the country is pushing nuclear power:
First, China's third-generation nuclear power technology has achieved substantive breakthroughs. All new nuclear power units under construction are equipped with third-generation technology, with significant improvements in both safety coefficients and power generation capacity. Moreover, China has an excellent safety record in nuclear power utilization, giving it the confidence to develop nuclear energy further.
Second, to achieve its dual carbon goals, China needs nuclear power to play a major role in energy conservation and emissions reduction, in addition to developing photovoltaic and other new energy sources.
Although nuclear power requires long investment cycles, its emissions reduction effects are considerable. Currently, nuclear power accounts for roughly 5% of China's electricity generation mix; by 2035, this share is expected to reach 10%.
Therefore, from a broader perspective, nuclear medicine is a shining jewel born from China's push to develop nuclear power. The biggest bottleneck in nuclear medicine development is the supply chain for radioisotopes — many isotopes need to be produced in reactors. The number of reactors a country has directly affects isotope supply.
Looking overseas, France is a major nuclear power nation. Novartis's radioligand therapy platform was built up primarily through its acquisition of Advanced Accelerator Applications (AAA), a French innovative drug listed company. We will also elaborate below on Novartis's exploration in the nuclear medicine field.
/ 03 / "A Romance Beyond the Age of the Universe" and the Long History of Nuclear Medicine
Before diving into nuclear medicine specifically, let's share some nuclear physics knowledge. Most relevant to nuclear medicine is the concept of radioactive decay in nuclear physics. Elemental transformation falls into three major categories: fusion, fission, and decay. Nuclear fission is mainly used for atomic bomb production; nuclear fusion is currently "hot," with people researching how to use controlled nuclear fusion to bring more clean energy.
Nuclear medicine, however, utilizes elemental decay. Decay refers to elements spontaneously emitting α, β, and γ particles, transforming from one element into another. Almost every element in the periodic table has radioactive isotopes.
A key concept in decay is half-life — the time required for the number of atomic nuclei of a radioactive isotope to decay to half its original amount. Different elements have half-lives ranging from very short to very long; the shortest may be just a few microseconds or even less.
A short half-life for a radioisotope means extremely high demands on the production, storage, and logistics of nuclear medicine.
CNNC once shared a typical nuclear medicine transportation scenario: "In the early hours of Saturday, radioactive raw materials arrive at the capital's airport. Professional transport vehicles arrive at the airport in advance, immediately transfer the cargo to production facilities upon receipt. According to relevant requirements, after 11 PM on Saturday, transport vehicles may enter Beijing's Sixth Ring Road, and only then can nuclear medicine depart from the production base for transport to airports or train stations. After receiving the cargo, transport vehicles immediately deliver to the hospital using the medicine, to ensure the hospital can administer it on time Monday morning."
Here's a fun fact: how long can an element's half-life be? Bismuth has the longest half-life — even 1 billion times the age of the universe. Scientists once believed bismuth was a stable element that didn't decay. Later they discovered its half-life is so long that it's extremely difficult to observe. So when people express love, instead of saying "until the seas run dry and the rocks crumble," they could say "even if bismuth decays."
Let's review the history of nuclear medicine development.
From humanity's first discovery of radioactivity in 1897 to today, more than a century has passed. Once people discovered radioactivity, they began wondering how to use it to treat disease. In 1941, iodine was first used to treat thyroid disease. Different human organs absorb radioactive materials to varying degrees — the thyroid readily absorbs iodine. Another element, strontium, tends to accumulate in bone, and was therefore used to treat metastatic bone tumors.
Nuclear medicine entered a period of rapid development only after 2000. In 2002, IDEC's Zevalin received FDA approval; this drug uses Yttrium-90 for radiolabeling to treat relapsed or refractory B-cell non-Hodgkin's lymphoma. In 2013, Bayer's nuclear medicine Xofigo came to market for treating prostate cancer that has spread to bone.
But it was Novartis that caused a sensation in the pharmaceutical world with nuclear medicine.
In 2018, Lutathera (lutetium Lu 177 dotatate), developed by a Novartis subsidiary, received FDA approval for treating a class of cancers affecting the pancreas or gastrointestinal tract — neuroendocrine tumors.
In 2022, another Novartis-developed drug, Pluvicto, came to market for treating metastatic castration-resistant prostate cancer (mCRPC).
In the history of nuclear medicine development, there hasn't yet been a single major breakthrough technology that detonated the industry. But through long years of continuous iteration and integrative innovation, nuclear medicine has advanced to where it is today. People are increasingly realizing the tremendous potential of nuclear medicine in cancer treatment.
04 The Advantages of Nuclear Medicine in Cancer Treatment
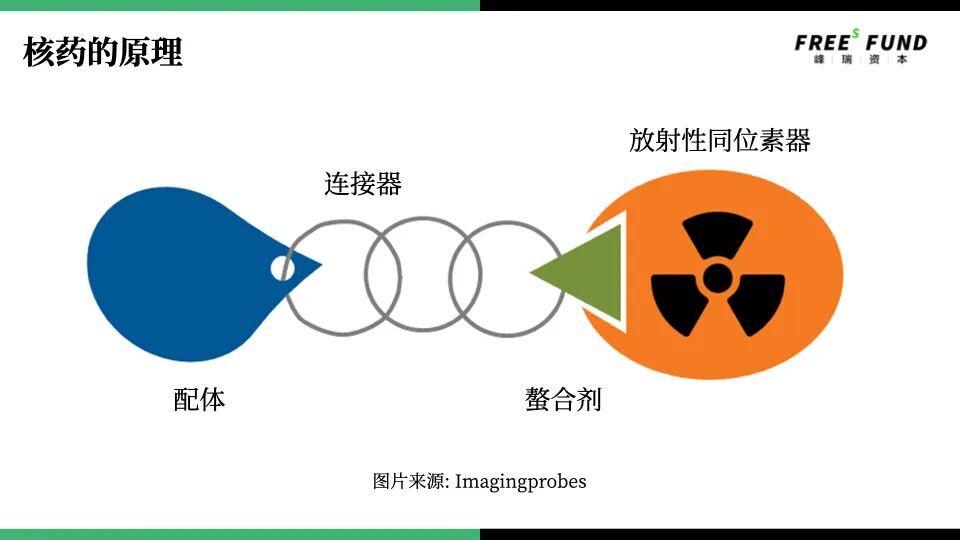
The principle of nuclear medicine is similar to that of antibody-drug conjugates (ADCs), which are currently in the spotlight. People use a linker to connect a targeting ligand with a toxin (payload), forming an ADC drug.
The success of ADC drugs has inspired enthusiasm for exploring "everything conjugation." People are thinking about how to use conjugation technology to develop new drug types.
Some startups are already exploring "everything conjugation." Genesis MedTech, a FreeS Fund portfolio company, is among the first batch of domestic biotech companies engaged in antibody-oligo conjugate (AOC) research, focusing on achieving extrahepatic targeted delivery of small nucleic acids through conjugation, and is a leading enterprise in this niche segment domestically.
Nuclear medicine replaces the toxin with a radioactive isotope; the isotope is bound to a chelator, then connected via a linker to a ligand, exerting therapeutic effects on targeted tissues or organs. The ligand in nuclear medicine can be a small molecule, peptide, or antibody.
But unlike antibody-drug conjugates, people don't want nuclear medicine to have too long a half-life in the body, so small molecules and peptides are more commonly used as ligands to shorten the half-life.
In the nuclear medicine field, Novartis's Pluvicto has become a "blockbuster" in the pharmaceutical market. In 2022, Pluvicto's sales reached $271 million. Novartis once optimistically projected the drug's peak sales would exceed $2 billion.
What exactly does this nuclear medicine do?
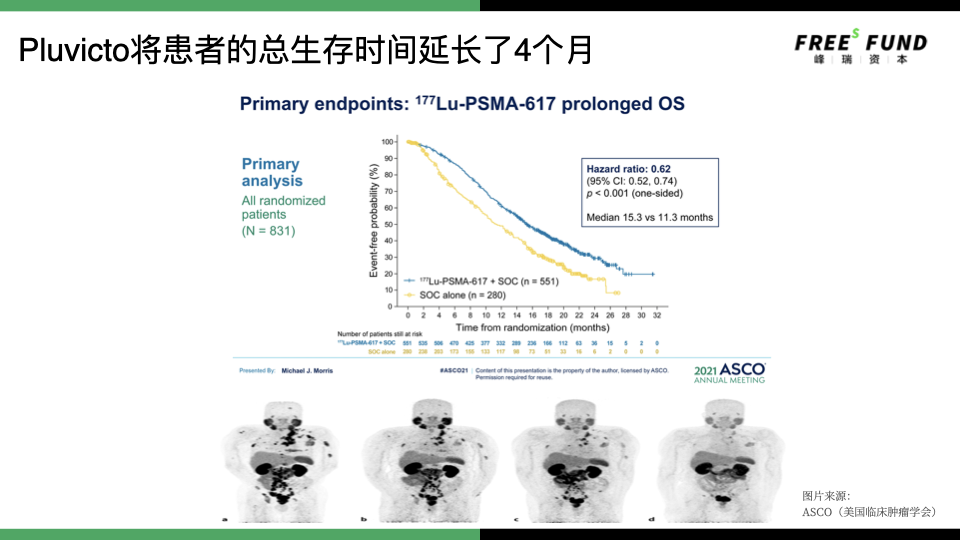
Let's look at the clinical data. The ultimate standard for evaluating drug efficacy is Overall Survival (OS, which can be understood as the time from disease onset to death).
Pluvicto changed patients' overall survival from 11.3 months before treatment to 15.3 months. Although it only extended survival by 4 months, for metastatic castration-resistant prostate cancer (mCRPC) — a disease that currently has virtually no treatment options — this is already quite meaningful.
In the field of cancer treatment, many problems have been solved or are on their way to being solved. What remains are the "hard bones" — advanced, metastatic, highly recurrent, drug-resistant tumors, and tumors in special locations.
Metastatic castration-resistant prostate cancer is one such hard bone. Prostate cancer is known as "the old man's cancer."
According to research by scholars including Fu Zhentao, 50 is the watershed for prostate cancer incidence; after 50, prostate cancer incidence begins to soar, and by 80, the probability of having prostate cancer is roughly 5,000 times that at 30.
WHO International Agency for Research on Cancer statistics show that in 2020, there were 1.414 million new cases of prostate cancer globally, with incidence ranking third after breast cancer and lung cancer.
But why do many people who get prostate cancer suffer no serious harm? Because prostate tumors grow very slowly; many men "live with the tumor," and may not even realize they have cancer until death.
According to research published in journals including Nature, some forensic pathologists performing autopsies on men find they had prostate cancer; the detection rate in the 60–74 age group is as high as 64%, significantly higher than other tumors in the same age group.
This slow spread also creates treatment difficulties. The usual way to kill tumors is chemotherapy, which exploits cells' rapid proliferation characteristics. But if cancer cells lie dormant in the body, gradually metastasizing to various parts, they become very difficult to kill.
If a patient develops metastatic castration-resistant prostate cancer (mCRPC), even when the body produces almost no androgen, the tumor and metastases continue to grow.
Nuclear medicine plays an important role in prostate cancer treatment; its tumor-killing mechanism differs from chemical drugs — it is physical killing. Nuclear medicine targets and approaches cancer cells, using α or β radiation to break DNA double strands and kill cells.
05 The Key to Nuclear Medicine Design: Precise Balance
Nuclear medicine design shares many similarities with ADC drugs — there are many considerations in selecting ligands, linkers, and isotopes. But nuclear medicine also has many unique characteristics. For example, in ligand selection: ADC drugs all use antibodies, but nuclear medicine ligands include small molecule peptides, antibodies, microspheres, and other forms.
Although antibodies are easily screened for and have good binding sites, they are large in size with long half-lives, and their penetration into tumors is limited. In drug design, we certainly don't want radioactive isotopes wandering around the body for a month or two, irradiating all the internal organs; rather, we want the nuclear medicine to precisely kill target cells and then be excreted from the body as quickly as possible.
If using an antibody as the targeting head, engineered design modifications to the antigen-binding domain or crystallizable fragment are needed to adjust antibody PK (pharmacokinetics) and obtain the optimal combination.
Currently, the most commonly used ligands in nuclear medicine are small molecules or peptides. Small molecules and peptides have advantages including small molecular weight, short blood half-life, and strong tumor penetration capabilities, but they also have certain renal toxicity. Additionally, it is difficult to screen small molecules and peptides for high-affinity, high-specificity molecules.
Similarly, the metabolic profile of nuclear medicine molecules in different tissues and organs is critical. Good drug design aims to have the isotope enrich and linger at the lesion site, while being metabolized and cleared from other tissues as quickly as possible.
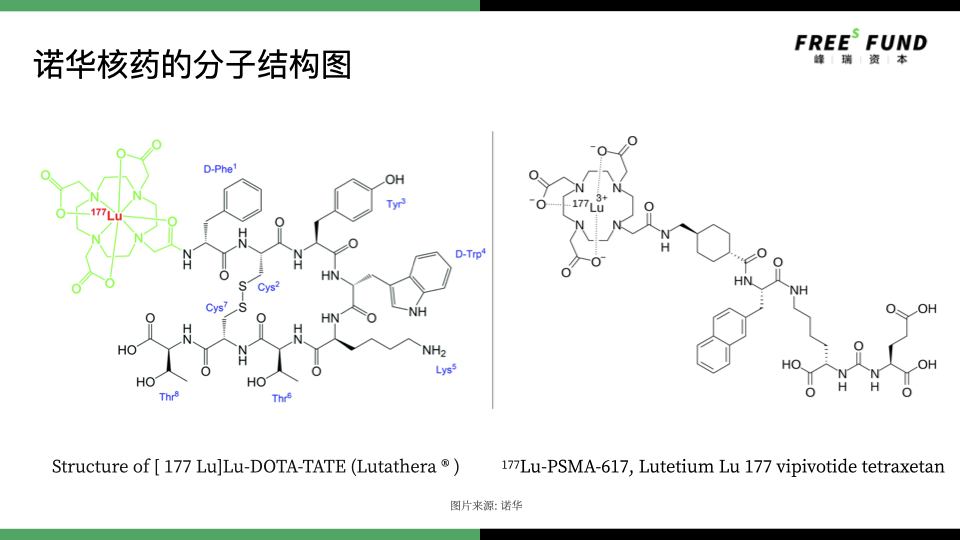
The image above shows the molecular structure of a nuclear medicine developed by Novartis, which uses small molecule peptides as ligands.
06 How Does Nuclear Medicine Achieve Personalized Quantitative Dosing?
In clinical practice, patients respond differently to the same drug. Even for identical diseases, different patients may require different medications, or if given the same drug, different dosages. But conventional drugs struggle to achieve individualized dosing, so the final optimized dose for approved drugs ends up being the greatest common denominator within the safety window. Nuclear medicine, however, is a physical therapy, so clinicians can model each individual patient and theoretically achieve personalized quantitative dosing — a genuine breakthrough.
Why can nuclear medicine enable individualized quantitative dosing?
Nuclear medicine is radioactive, so it can be combined with clinical PET-CT (computed tomography) to quantitatively model and numerically calculate lesion target areas. Because both PET-CT and nuclear medicine are radioactivity-based, the CT's measured radiation absorption values for tissues and organs can be directly used for quantitative nuclear medicine dose calculations.
Before diagnosis, nuclear molecular imaging can reveal the distribution of lesions in the body. During diagnosis, combined with PET-CT, it can image and quantify the distribution and changes of radioactivity in different tissues and organs.
Then, through dosimetry, researchers study the radioactivity or absorbed dose in various tissues and organs as pharmacodynamic evaluation indicators. The absorbed dose to target lesions can be calculated using data models in specialized software (such as OLINDA).
Of course, to truly achieve personalized quantitative dosing, further clinical accumulation of extensive tissue and organ absorption and metabolism data is needed for calibration before personalized precision dosing can finally be realized.
07 Why Is Nuclear Medicine Development Constrained by Supply Chains?
Beyond ligand selection, the radionuclide itself critically impacts nuclear medicine. Earlier, when discussing decay, we noted that radioactive decay of certain atoms produces atoms of another nuclide, releasing particles such as alpha particles, beta particles, or neutrinos.
Alpha and beta particles differ substantially in energy and range. Alpha particles have very high energy but extremely short range — only a few micrometers, roughly the size of one or two cells. Beta particles have relatively lower energy but longer range, on the millimeter scale.
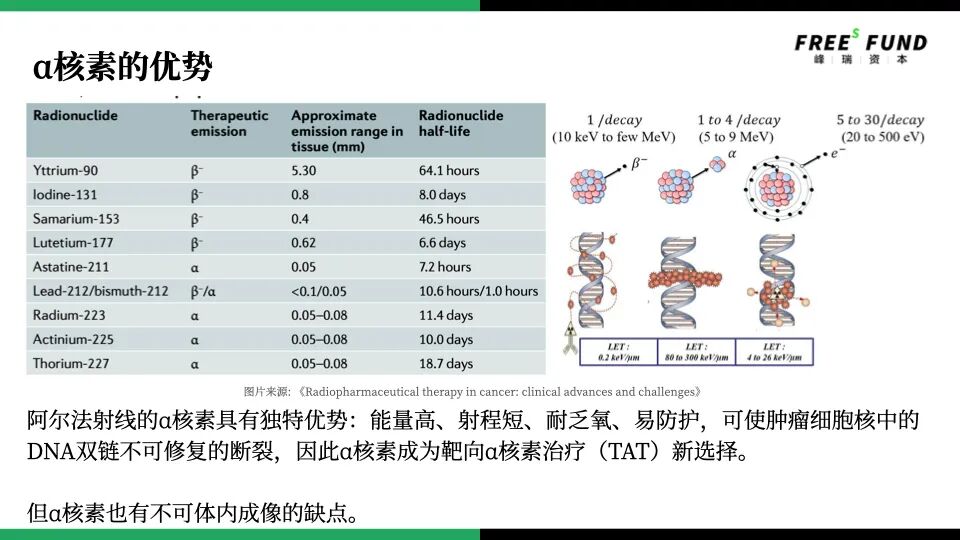
By comparison, alpha particles show more promise. Because their interaction distance is so short, they avoid damaging surrounding tissue. Additionally, alpha particles carry high energy — a single alpha particle can break both DNA strands, while beta particles can only break one. Cells have self-repair mechanisms; when only one strand is broken, they can quickly repair it.
If beta particles are used as the radionuclide, sufficient quantity is needed to break DNA strands. Alpha particles have disadvantages too — their biggest weakness is that they cannot be imaged in vivo because their range is too short to be captured, though solutions are emerging.
The production methods for the two particle types also differ significantly. Producing alpha particles requires nuclear reactors, which creates enormous difficulties for nuclear medicine R&D and production. The number of nuclear reactors worldwide is very limited. Producing beta particles only requires accelerators.
Overall, nuclear medicine has not developed rapidly. This slow progress is closely tied to constrained radionuclide supply chains. In the periodic table, elements with higher atomic numbers and more neutrons typically require nuclear reactors for radionuclide production.
Globally, radioactive nuclides depend on a tiny number of research reactors for production. These research reactors were built long ago, have high maintenance costs, low annual output, and face safety challenges with waste disposal. Many reactors are scheduled to close around 2025, causing permanent production reductions.
Moreover, in recent years, nuclear anxiety has spread across many regions globally. On one hand, people want to prevent nuclear weapons proliferation; on the other, incidents like Chernobyl and Fukushima have led some countries to shut down many nuclear power plants. In April 2023, Germany closed its last three nuclear power plants, formally ending its "nuclear power era." As early as 2011, due to public opposition, the Italian government announced it would abandon nuclear energy.
08 Theranostics and Combined Internal-External Radiation
Having covered nuclear medicine, let's turn to nuclear molecular imaging. Over the past decade-plus, CT and PET-CT have advanced rapidly. When combined with nuclear medicine, these technologies can reveal more comprehensive tissue structure and molecular biology information.
Nuclear medicine can use the same targeting moiety with different radionuclides to combine radionuclide imaging with internal radiotherapy. For example, Novartis's Pluvicto (177Lu-PSMA-617) can be paired with 68Ga-gallium imaging to visualize tumor distribution in the patient's body, helping doctors comprehensively analyze whole-body tumor burden before surgery and enabling postoperative monitoring, quantitative analysis, and evaluation.
Beyond its widespread use as a molecular imaging virtual biopsy for tumors, nuclear medicine also serves as the diagnostic gold standard in neurobiology — for instance, in diagnosing Alzheimer's disease — where clinical practice requires PET-CT combined with nuclear medicine molecular imaging to detect and diagnose various brain diseases.
Why is nuclear medicine molecular imaging established as the gold standard in neurobiology?
Because from a purely quantitative perspective, it's difficult to distinguish normal individuals, those with mild cognitive impairment, and Alzheimer's patients based on quantity alone. Beyond quantification, you need to examine brain tissue structure and functional distribution. For example, the hippocampus shows substantially different distributions in mild cognitive impairment and Alzheimer's patients. Relying solely on single-molecule quantitative information may not capture the full picture.
Beyond the advantage of theranostics, external beam radiation has advanced rapidly in recent years with proton and heavy ion therapies, and even breakthrough technologies like biologically guided radiotherapy have emerged.
Biologically guided radiotherapy fully integrates PET-CT with proton accelerators. During PET-CT scanning, the equipment can image in real-time, telling you the tumor's location, while simultaneously using the proton accelerator to deliver radiation for precise tumor targeting.
The synchronous development of large-scale equipment like proton accelerators alongside nuclear medicine is making combined internal-external radiation treatment protocols increasingly feasible. In the future, external radiation may address large tumor masses while nuclear medicine eliminates small or free-floating cancer cells.

09 Summary: Advantages and Challenges Facing Nuclear Medicine

To summarize, why is nuclear medicine becoming increasingly important, and what are its advantages?
The core advantage of nuclear medicine is precision therapy, specifically manifested in four ways:
First, distinctive visualized theranostics. As we just discussed with biologically guided radiotherapy, the detection and treatment process is integrated.
Second, achieving personalized precision dosing. Nuclear medicine can provide quantitative, precise evaluation and medication for patients across pre-diagnosis, mid-diagnosis, post-diagnosis, and post-surgical stages.
Third, physical killing offers advantages against drug resistance and for combination therapy. Nuclear medicine physically destroys cancer cells, giving it major advantages over traditional drugs regarding resistance. It can also be combined with chemotherapy and immunotherapy, as these approaches have different killing mechanisms.
Fourth, combining internal and external radiation. For some late-stage cancer patients, tumor cells or even tumor masses may be distributed throughout the body, making surgery difficult and traditional drugs hard-pressed to cure. In such cases, external radiation can be used with proton accelerators to destroy masses, while any remaining tumor cells can be treated internally with nuclear medicine. This combined approach is already being used clinically.
Nuclear medicine still faces considerable challenges today:

First, high regulatory barriers. All aspects of radioactive drug operation, transportation, import, production, and use are strictly controlled by relevant authorities, including drug regulatory agencies, the Commission of Science, Technology and Industry for National Defense, transportation departments, health commissions, and customs.
Second, tight radionuclide supply chains. Due to the scarcity of domestic medical radionuclide production reactors, supply basically depends on imports. Additionally, radionuclides have half-lives — once expired, they become unusable.
Third, insufficient nuclear medicine talent supply. Nuclear medicine is an interdisciplinary field involving diverse knowledge areas, but China has few people with interdisciplinary backgrounds and industry experience. The earliest active nuclear medicine industry professionals mostly came from universities and hospitals.
Despite these layered challenges, developing nuclear medicine is "the right thing, not the easy thing." The potential of nuclear medicine in tumor treatment and brain disease diagnosis and treatment is evident to all. We look forward to meeting more entrepreneurs dedicated to advancing nuclear medicine.
Engagement Giveaway What changes do you think "nuclear" has brought to our lives? Share your thoughts in the comments. The 5 most thoughtful commenters will each receive a copy of Life Atomic, a work that details how nuclear energy was applied to science and medicine after World War II. We look forward to your sharing.

A Debate: Two Investors From Different Directions on How They View GPT | FreeS Research Institute
Every Brain Is a Unique Little Universe | FreeS Fund World Autism Awareness Day Special
How to Invest in Biotech in 2023? | FreeS Research Institute
Talking AIGC: How Can Vertical Tracks Find Opportunities in This AI Wave? | FreeS Fund Dialogue
Star the FreeS Fund WeChat Official Account for timely business insights.