FreeS Fund Report 15: The Life Gamble — The Risk-Filled Journey of Drug R&D | Frees Fund

The Ideals and Persistence Behind a 3% Success Rate.

In FreeS Report Issue 15, we're talking about drug development — a field with a mere 3% success rate.
During World War II, the discovery and deployment of penicillin saved countless wounded soldiers. By helping the human body fight bacterial infections, it became known among troops as the "lifesaving drug" and, in Churchill's eyes, "the greatest invention of World War II."
Gleevec, the miracle drug featured in the film Dying to Survive, delivers complete responses in over 96% of patients with newly diagnosed chronic myeloid leukemia, pushing five-year progression-free survival from 64% to 83% — nearly indistinguishable from normal life expectancy.
Breakthroughs like these have cured diseases, elevated quality of life, and extended human lifespan. Yet across more than a century of drug development history, formidable challenges remain unsolved — Alzheimer's among them — and tragedies have never been absent. Thalidomide's teratogenic effects, for instance, led to the "seal baby" disaster.
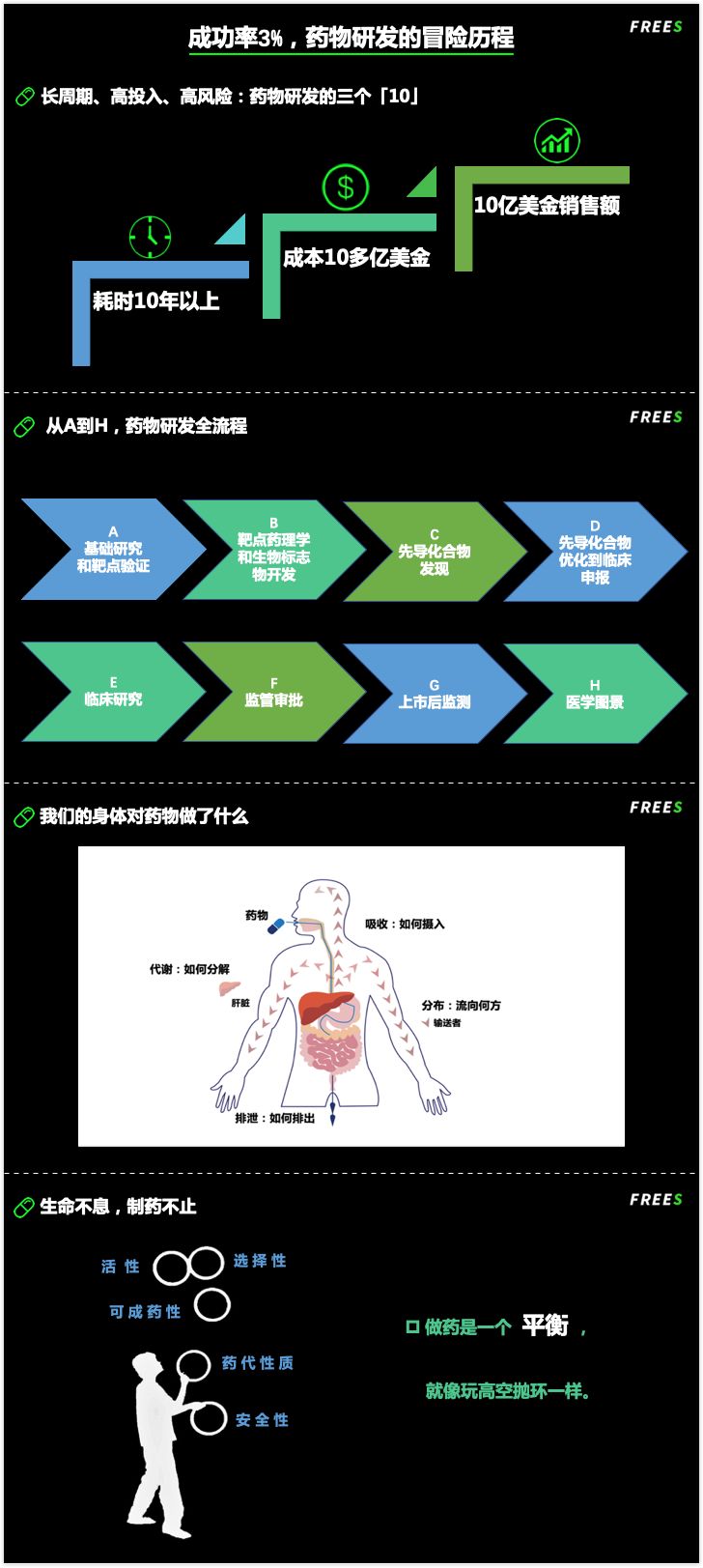
Making drugs is like juggling rings at altitude: you must find balance among activity, selectivity, druggability, metabolism, and safety. In pursuit of that equilibrium, innumerable preclinical studies and clinical trials have crashed and burned; hundreds of millions of dollars evaporating is simply par for the course.
This report takes a popular-science approach to walk you through pivotal events and milestones in pharmaceutical history, decoding the drug development journey. You'll learn:
- Why is drug development considered a long-cycle, high-investment, high-risk gamble?
- Why is developing a drug so difficult, and why do so many medicines carry astronomical price tags?
- What contributions have mice, rats, dogs, monkeys — plus rabbits, pigs, groundhogs, ducks, and more — made to drug development as model organisms?
- When we swallow a pill, what does our body do to the drug, and what does the drug do to our body?
If entrepreneurship in drug development means burning cash and taking bold risks, then early-stage investment in this domain is equally expensive, protracted, fraught with risk and uncertainty. Yet beyond commercial considerations, supporting pharmaceutical innovation carries profound social meaning. FreeS Fund maintains a long-term conviction in healthcare investments spanning novel drug R&D, medical devices, in-vitro diagnostics, and medical services — with ample patience and resources to accompany startups through their growth. We look forward to engaging with more entrepreneurs in the medical field.

The Drug Development Journey
By Yikai Wang (yikai@freesvc.com)
/ 01 /
Life Goes On, So Does Drug Making
Among the world's top 10 best-selling innovative drugs in 2017 and 2018, eight were biologics (seven antibody drugs and one fusion protein) and two were small-molecule drugs.
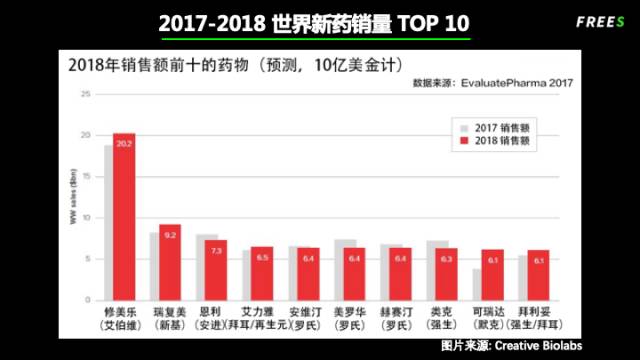
Meet the "blockbusters" — drugs generating over $1 billion in annual sales. Humira (adalimumab) reigned supreme with $18.4 billion in 2017 sales. This biologic, developed by AbbVie, held the top spot. In second place came Revlimid (lenalidomide), a small-molecule drug raking in $8.1 billion, developed by Celgene. Third was Enbrel, from Amgen...
Regrettably, not a single blockbuster has yet emerged from a Chinese company.

FreeS Fund Perspective
Healthcare spending tied to individuals and families has risen steadily in recent years. In 2015, Chinese residents spent 4 trillion yuan on medical care, growing at roughly 20% annually. Diagnosis and treatment of major diseases account for the bulk of this spending, with imported drugs and medical devices representing the largest slice. Addressing accessibility and affordability requires not only curbing unreasonable costs in distribution, but also doing everything possible to localize key technologies and products.
While biologics dominate current R&D and sales, the history of modern drug development began with small-molecule chemistry.
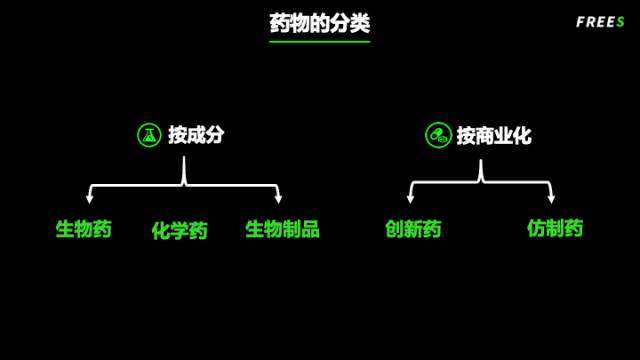
By composition and structure, drugs broadly fall into:
Small-molecule drugs: Single, well-defined active ingredients, typically with molecular weight below 1,000 Daltons
Biologics: Antibodies, proteins/peptides, and nucleic acid drugs, typically with molecular weight far exceeding 1,000 Daltons
Biological products: Non-single-component vaccines, viral, and cellular therapies
By R&D and commercialization stage, drugs divide into innovative drugs and generics:
Innovative drugs: Proprietary drugs with independent intellectual property
Generics: Copies of innovative drugs, permitted for market entry only after the original drug's patent protection expires
/ 02 /
From the Mid-19th Century to Today:
The Evolution of Drug Discovery Approaches
Using small-molecule chemical drugs as our example, let's review three phases of pharmaceutical R&D.
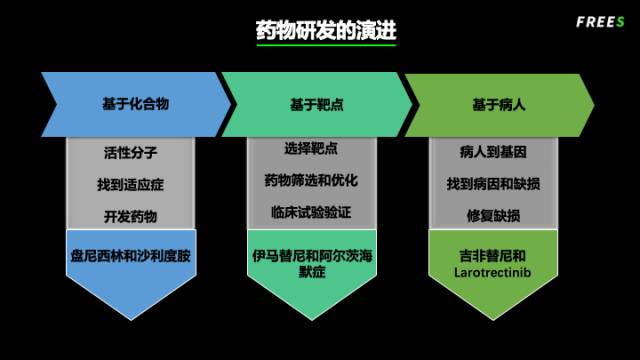
Phase one: the compound-based era, roughly from the rise of the pharmaceutical industry in the mid-19th century through the 1950s–60s before molecular biology became widespread. There was no concept of "targets" — only compounds extracted from nature or synthesized artificially. Researchers screened these for biological activity, then figured out what diseases they might treat. (See: The Penicillin Miracle; The Thalidomide Tragedy and Comeback)
Phase two: the target-based era. This began in the 1970s–80s, emerging alongside molecular biology, high-throughput screening, and combinatorial chemistry. The starting point was selecting a biologically well-understood "target," screening for compounds that could modulate it, optimizing for druggability, and ultimately validating through clinical trials. (See: The "Miracle Drug" Gleevec; The Alzheimer's Gamble)
Phase three: the patient-based era. This door opened with the completion of the Human Genome Project in 2000. The core principle: start from the patient, identify the defect, then develop treatments targeting that defect — with or without reliance on specific targets. Personalized medicine, precision medicine, and gene therapy are all buzzwords of this era. But this phase has only just begun; the road ahead remains long. (See: Gefitinib — A Gift from God to Eastern Populations; The Success of "Basket" Trials)
/ 03 /
Miracles and Regrets in Pharmaceutical History
Each phase has brought breakthroughs and setbacks; tragedy and triumph have always intertwined.
The Penicillin Miracle
Penicillin's discovery stands as the classic case from the compound-based era.
▲ The "lifesaving drug" for WWII soldiers.
In 1928, British bacteriologist Alexander Fleming noticed something peculiar: a new mold whose surrounding Staphylococcus colonies had dissolved, unable to grow. Colleagues dismissed the contaminated petri dish as waste, but Fleming saw something worth investigating. He eventually confirmed an entirely unknown substance with extraordinary bactericidal power. Secreted by Penicillium mold, it was named penicillin.
Fleming, however, failed to purify the substance. It wasn't until 1941 that Howard Florey and Ernst Chain achieved isolation and purification, with large-scale production following in 1942 and regulatory approval in 1943.
Penicillin's discovery and use in World War II saved untold lives. Advances in antibiotics more broadly would dramatically extend human life expectancy.
The "Miracle Drug" Gleevec
In the target-based drug development era, one recently prominent drug is Gleevec (the real-world inspiration for "Glenin" in Dying to Survive). Approved in 2001 for chronic myeloid leukemia treatment:
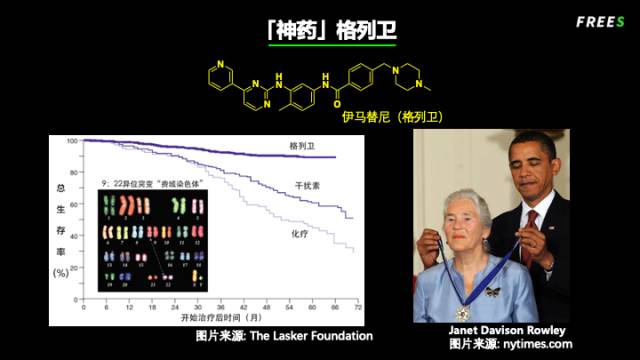
Gleevec is considered one of the miracles in pharmaceutical history. In the 1960s, Peter Nowell, a professor of pathology at the University of Pennsylvania, discovered that in cancer cells from patients with chronic myeloid leukemia, chromosome 22 was conspicuously shorter. In 1973, University of Chicago professor Janet Rowley found that this shortening was caused by chromosomal translocation — a partial exchange between chromosomes 9 and 22.
In 1987, scientists further discovered that this chromosomal exchange had created a new protein called BCR-ABL, which does not exist in normal cells. The emergence of this new protein caused uncontrolled cell division, triggering cancer.
Fortunately, beginning in the 1980s, after a series of designs and modifications, researchers discovered compounds that could inhibit BCR-ABL and kill cells carrying this mutation. In 2001, this drug was approved and marketed under the generic name imatinib and the brand name Gleevec.
Patient survival curves prove that this drug deserves its "miracle" reputation. In over 96% of newly diagnosed chronic myeloid leukemia patients, cancer cells completely disappeared after taking the medication. Compared with traditional therapies, Gleevec improved patients' five-year progression-free survival rate from 64% to 83% — nearly indistinguishable from normal life expectancy.
Beta-Amyloid: The Alzheimer's Gamble
As target-based drug development took center stage, humanity reaped both gifts and setbacks.
To this day, Alzheimer's disease (commonly known as "senile dementia") remains unconquered, though our efforts have never ceased. In 1984, scientists discovered numerous beta-amyloid plaques and neurofibrillary tangles in the brains of Alzheimer's patients. Subsequently, mainstream academia concluded that beta-amyloid accumulating inside the brain was the culprit behind Alzheimer's.
Thus, many bet that inhibiting beta-amyloid production or reducing its quantity would treat Alzheimer's. Global pharmaceutical giants including Johnson & Johnson, Eli Lilly and Company, and Merck Group have invested — or continue to invest — heavily in pathways related to beta-amyloid.
Regrettably, to date, none of this R&D has achieved substantive progress. Countless clinical trials have failed, and tens of billions of dollars have gone down the drain. In 2016, Eli Lilly announced trial failure. On Valentine's Day 2017, Merck announced it had not achieved positive results. In January 2018, Pfizer announced it was abandoning related research. The most expensive hypothesis and target in drug development history remains on the path to being proven or disproven...
The key to success in target-based drug development is whether the target is cause or effect in the pathological process. BCR-ABL is the cause, thus making Gleevec possible. As for the relationship between beta-amyloid and Alzheimer's, more voices now believe the former is the effect.
▍Gefitinib — A Gift from God to Easterners
As the era of patient-based drug development stumbled forward, gefitinib undoubtedly became a benchmark, and also marked the first time Chinese clinical oncology research stepped onto the world stage.
In the 1980s, as molecular biology continued to develop, researchers discovered that the EGFR signaling pathway was activated in lung cancer patients. Following the target-based development approach, the small-molecule drug gefitinib was developed to target this protein. It was approved in Japan in 2002 under the brand name Iressa. In 2003, Iressa was approved in the United States, but in 2005 the FDA withdrew this approval. The reason: the FDA found insufficient evidence that gefitinib significantly extended patients' lives. At the time, data showed gefitinib extended survival by an average of only two weeks. This also made the value of targeted cancer therapy heavily criticized and questioned.
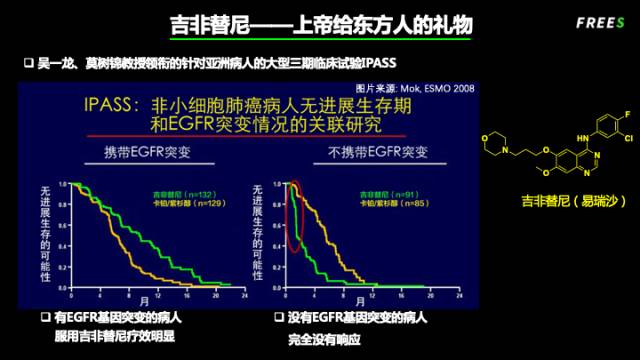
However, Chinese scholars were unwilling to accept this. In retrospective analyses, Dr. Yilong Wu in Guangzhou and Dr. Tony Mok in Hong Kong discovered that while gefitinib's treatment effect was indeed mediocre in lung cancer patients generally, the response rate was relatively high among Asian women with no smoking history — these patients often carried EGFR gene mutations. So they conducted a landmark clinical trial called "IPASS" across China and Asia, screening patients by genetics to identify those carrying EGFR mutations and test the drug's efficacy.
This study shocked the world. Compared with chemotherapy, EGFR mutation-positive patients taking gefitinib saw median survival extend from 6-7 months to 12 months; for patients without EGFR mutations, survival actually shortened. It was precisely because of this study that the FDA re-approved gefitinib in 2015 for treating patients with EGFR mutations.
▍The Success of "Basket" Trials
Finding causes from patients and developing drugs targeting those causes is the development trend of the third stage, and is slowly becoming reality. At the 2018 ASCO conference, LOXO announced a globally eye-catching clinical research result, writing a vivid chapter in the history of precision medicine.
In nearly all common tumors, Trk protein fusion mutations exist, though at low frequencies. Combining Trk-related mutations across different tumors, over a dozen new proteins are produced. If these new proteins could be inhibited like imatinib inhibits BCR-ABL, tumor growth could be suppressed.
With this understanding of cause, the remaining questions simplified to two aspects: first, could a compound be found that simultaneously inhibits these dozen-plus different proteins; second, since the proportion of patients carrying this mutation in each tumor type is small, how could enough patients be found for clinical trials.
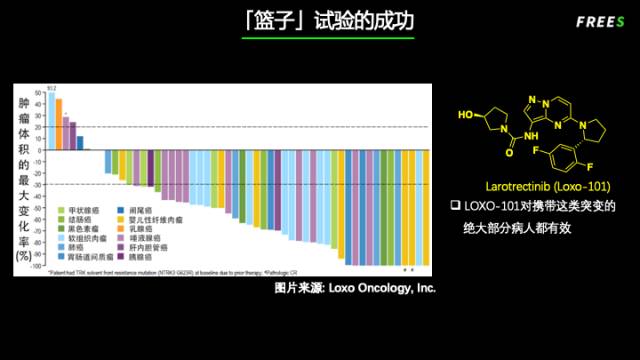
For the first question, fortunately, these dozen-plus proteins are all tyrosine kinases, and LOXO found the small molecule larotrectinib, which inhibits only these kinases without affecting others.
For the second question, LOXO designed a so-called "basket" trial: through genetic sequencing, identifying patients carrying this type of mutation across all tumor types. Whether gastric cancer, lung cancer, or breast cancer — all were treated together. Clinical results were outstanding: the vast majority of patients saw their tumors shrink or even disappear! LOXO's stock surged from $116 to $208 within a month.
The importance of this "basket" trial can be summarized in three points: precision, efficacy, and economy. Starting from patients' genetic level is precision; targeting pathological causes brings efficacy; using the "basket" approach to increase patient numbers is economical (ensuring sufficient market size).
The Tragedy and Comeback of Thalidomide
Next, the story of thalidomide spanning 60 years.
When it was first synthesized, humanity was still in the compound-based drug development era. Its brief popularity caused countless tragedies. It topped chemical drug sales in the target-based development era, yet its target remained elusive. When its target was finally discovered, a new direction was opened, providing powerful tools for patient-based drug development.
Thalidomide's teratogenic effects causing widespread "phocomelia" (seal limb) tragedies represent one of the darkest chapters in pharmaceutical history.
▲ The "phocomelia" tragedy caused by "Contergan."
In 1953, Ciba — predecessor of Novartis — synthesized the compound thalidomide, intending it as an antibacterial agent, but it proved ineffective. A West German pharmaceutical company discovered that thalidomide had certain sedative and hypnotic effects, and could significantly suppress morning sickness in pregnant women.
In October 1957, thalidomide was officially launched in the European market, packaged as "an anti-nausea drug for pregnancy with no side effects whatsoever," and given the name "Contergan." Thalidomide quickly became popular across Europe, Africa, Australia, and Latin America, with large numbers of pregnant women using it.
Yet within just one year, European doctors noticed that the birth rate of deformed infants (phocomelia, with underdeveloped upper limbs) in their regions had clearly risen, and identified this deformity as closely related to thalidomide. In 1961, thalidomide was recalled from markets worldwide, and formally withdrawn in 1963. By the time of recall, approximately 15,000 babies worldwide had been affected. German company Chemie Grünenthal consequently paid 110 million Deutsche Marks in compensation and was forced into bankruptcy.
While thalidomide was sweeping through Europe, the FDA had rejected this drug's marketing application. FDA officer Frances Kelsey, who was responsible for reviewing this application, noticed significant gaps between thalidomide's human and animal trial data. She rejected approval on the grounds of unclear pharmacological activity and substantial species differences. Despite pressure from the pharmaceutical company, she held firm, preventing the tragedy from occurring in the United States.
Later research discovered that the thalidomide molecule is a pair of mirror-image isomers: one isomer has sedative effects, while the other causes deformities. In the body, these two isomers can interconvert, so even taking only the sedative isomer would result in half converting to the teratogenic one inside the body — meaning the side effects were unavoidable.
The thalidomide tragedy directly led to passage of the Kefauver-Harris Amendment. Its main provisions: establishing a drug advertising application system; requiring all drugs to submit safety and efficacy proof to the FDA; establishing procedures for new drug research and approval; requiring drug manufacturers in the U.S. to implement GMP.
Like two sides of a coin, while this legislation raised the threshold for drug registration and marketing applications, it also reduced the quantity and speed of new drug approvals. From 1962 to 1983, no generic drugs came to market. Additionally, because generic drugs also needed clinical trials to prove efficacy, this led to expensive drug prices and poor accessibility.
It was not until 1984 that the FDA enacted the Hatch-Waxman Act, introducing the concept of generic drugs and relaxing generic drug thresholds, which solved drug accessibility and cost issues. Today, approximately 80% of prescriptions in the U.S. market are generic drugs, yet generic drug sales account for only 30%.
The "phocomelia" tragedy thalidomide caused was only the beginning of its story. After a period of silence, the drama of "redemption" began to unfold.
Because of its immunosuppressive activity, on July 16, 1998, the FDA approved thalidomide for the treatment of erythema nodosum leprosum. Then, thanks to its anti-angiogenic properties, in 2006 the FDA approved thalidomide in combination with dexamethasone for patients with newly diagnosed multiple myeloma. Later, Celgene discovered that a thalidomide derivative, lenalidomide, had even greater anti-tumor activity. In 2008, the FDA approved lenalidomide plus dexamethasone for multiple myeloma patients who had received at least one prior therapy. To date, lenalidomide has been approved for three oncology indications, with dozens of clinical trials underway, generating $8.1 billion in annual sales.
But the story doesn't end there. Although we had entered the era of target-based drug discovery, it's ironic that neither thalidomide nor lenalidomide's actual target had been identified.
It wasn't until 2011 that researchers discovered their target was cereblon, an E3 ligase involved in protein degradation. Leveraging this mechanism, scientists realized that small molecules could selectively degrade disease-causing proteins — a function previously achievable only through siRNA or CRISPR technology. Starting in 2014, small-molecule protein degraders became a hot new area; interested readers should look into PROTAC. And it all traces back to that very simple molecule — thalidomide.
From the "phocomelia" tragedy to applications in oncology, to opening up an entirely new research direction — more than 60 years in total, and the story continues...
FreeS Fund Perspective (freesvc)
Drug development is an expensive, lengthy, complex journey fraught with risk and uncertainty. Looking back at nearly two centuries of pharmaceutical history from where we stand today, the foundation lies in innovations in tools and methods and gains in efficiency; the key is understanding biological processes and disease. Of course, the core driving force behind all of this is humanity's longing for immortality.
The Nine Deaths of Drug Development
Drug development is a long-cycle, high-investment, high-risk adventure. Three "10s" are commonly used to describe this journey: "10 years" in duration, "10 billion" dollars in cost (in recent years, bringing a new drug to market takes longer than 10 years and costs far more than $10 billion), and of course a third "10" to measure the outcome — "10 billion" dollars in sales.
Why is this the case?
To understand the difficulty of drug development, you first need to understand the process, which is extraordinarily complex, as shown below:
▍From A to H
From early-stage R&D to market approval, the steps and processes are so extensive they can be listed from letter A to H.
A, first comes basic research. This involves starting from patients, clinical pathology, and statistical data to identify and validate potential targets.
B, pharmacology and biomarker development. This includes pharmacological and druggability studies of the target, as well as biomarker research related to the target and prognosis.
C, lead compound discovery. Lead compounds are biologically active compounds obtained through various approaches and methods, typically screened in vitro, and used for further structural modification and optimization.
D, lead compound optimization, preclinical candidate confirmation, preclinical studies supporting regulatory filings, and CMC (Chemistry, Manufacturing, and Controls). In this stage, potential drug candidate molecules are selected and subjected to systematic pharmacodynamic and toxicological studies. Samples to support clinical studies must also be manufactured under Good Manufacturing Practice (GMP) conditions.
E, clinical studies. This mainly involves clinical trials, including Phase I, Phase II, and Phase III trials. Each phase has different objectives and scales.
F, regulatory approval. The primary goal at this stage is to file for drug registration and marketing authorization. In the U.S., applications go to the FDA; in Europe, the审批单位 is the EMA; in China, applications are submitted to the National Medical Products Administration (NMPA).
G, post-market surveillance. This involves monitoring all information related to the drug after launch, including efficacy, safety, ethnic differences, off-label use, and so on.
H, medical landscape. This includes competitive positioning, pricing strategy, market share, physician education, and more. These determine the commercial success of the drug.
AstraZeneca summarized the above drug development process into five "Rights": right target, right tissue, right safety, right patient, and right commercialization. Using these five "Rights" to guide its internal R&D and decision-making, and after five years of practice, the company raised its project success rate (completion of Phase III trials) from 4% to 19% — far above the industry average of 3%. This was no easy feat.
In the A-to-H process, stage E, clinical trials, represents the largest investment and the highest risk of failure. To reduce failure rates, extensive preclinical research is needed to mitigate risks for the clinical stage. Below, we'll discuss what factors preclinical research must consider and what obstacles it must overcome.
The Long Journey of a Drug Through the Human Body
After oral administration, two things are generally considered most important for a drug to exert its effect. The first is pharmacokinetics (PK) — what the body does to the drug. The second is pharmacodynamics (PD) — what the drug does to the body.
Let's start with pharmacokinetics. Follow along as we take a trip through the body with an oral medication.
After a pill is swallowed, it first disintegrates in the stomach, releasing its compounds. It then moves with gastric peristalsis into the intestines. The intestine is the primary organ of absorption, with a vast surface area, and this is where most drug absorption occurs. As it passes through the intestinal wall, intestinal cells metabolize the drug. After passing through the intestine, it enters the liver via the hepatic portal vein. The liver is the most important organ for metabolic detoxification, specialized in clearing foreign molecules. It primarily modifies drug molecules through metabolic enzymes in hepatocytes, inactivating them for excretion. Only drug molecules that survive without being extracted or modified by the liver finally reach the heart and are transported throughout the body via the bloodstream. This is the absorption process.
As the drug circulates through the bloodstream, it diffuses into nearly all organs and tissues. This process is called distribution.
Whenever the drug passes through the liver during its continuous circulation, a portion is modified by metabolic enzymes in liver cells. This process is called metabolism.
Eventually, the drug or its metabolites are excreted via bile into the intestine and eliminated in feces, or filtered by the kidneys and excreted in urine. This is the excretion process.
Take gefitinib, mentioned earlier. After oral administration, it must be stable enough to be absorbed, not metabolized too quickly by the liver, distribute to the lungs, enter lung cancer cells, and approach its target EGFR — only then has it truly reached its destination and begun to exert its effect on the body. It must also maintain sufficient duration and concentration to be effective, what we commonly call drug exposure. Typically, adequate exposure is required for therapeutic effect.
Then pharmacodynamics takes the stage, focusing on what the drug does to the body. After reaching the vicinity of its target, at what concentration can it inhibit how much of the target's activity? How much inhibition is needed for pharmacological effect? How long must inhibition be sustained? What efficacy could be achieved with complete 24/7 inhibition? And so on.
Beyond pharmacokinetics and pharmacodynamics, toxicity must also be considered. For example, does inhibiting this target in normal tissues and organs cause side effects? Does the drug molecule affect other unintended targets, causing toxicity? Are the drug's metabolites toxic? And so forth.
How the body processes the drug is the foundation; what the drug does to the body — positive effects are efficacy, negative effects are toxicity — combined, these allow identification of a so-called therapeutic window: a drug where the benefit of treating the disease outweighs the harm to the body.
From Model Animals to Humans
To address the questions of drug metabolism, efficacy, and toxicity raised above, and to find a drug with a therapeutic window, yet without testing every candidate molecule in humans, extensive animal testing is required. This brings us to model animals in drug development.
Commonly used model animals include mice, rats, dogs, and monkeys; less commonly used are rabbits, pigs, groundhogs, ducks, and others.
Currently, the ability to predict drug metabolism using model animals is relatively high and the most accurate. In terms of toxicity, model animals' predictive ability is moderate, because significant differences exist between humans and animals. For efficacy prediction, results are generally poor, because animal models differ substantially from humans in disease mechanisms and progression.
For example, the American Association for Cancer Research (AACR) annual meeting consistently reports numerous promising results — "another type of tumor completely cured in mice" — yet at the American Society of Clinical Oncology (ASCO) annual meeting, truly major breakthroughs are rare. This indirectly reflects the poor translational predictive ability from mouse tumor models to humans.
As understanding of disease deepens and gene-editing tools continue to evolve, building animal models based on disease etiology to improve translational and predictive capability is a pressing pain point and challenge in current preclinical research.
The Preclinical Optimization Process for Small-Molecule Drugs
Before a drug candidate molecule enters clinical trials, it must go through multiple rounds of optimization cycles. In this process, what medicinal chemists can change is the molecular structure — using in vitro evaluation and in vivo assessment in model animals to verify whether structural changes improve upon the original in certain desired ways. Based on this, further structural modifications and validation are performed... This cycle must repeat dozens of times before a compound with acceptable properties in all aspects can be identified as a drug candidate.
This optimization loop involves three interlocking relationships: structure-activity (efficacy), structure-property (drug-likeness and metabolism), and structure-toxicity.
Beyond experimental testing, computation and AI can help across all three. For structure-activity relationships, which involve small-molecule-protein interactions, knowing a protein's structure enables computer-aided drug design to screen out obviously poor candidates early. For structure-property and structure-toxicity relationships, decades of accumulated data and experience can be leveraged — and with big data and machine learning, predictive accuracy keeps improving.
Tool innovation and efficiency gains in these areas have become a major research focus in both academia and industry in recent years.
FreeS Fund Perspective (freesvc)
Drug discovery is like juggling rings at altitude — you need to balance activity, selectivity, drug-likeness, metabolism, and safety. Change the molecular structure, and everything changes with it. It's a deeply complex process.
Closing
The molecules that survive this gauntlet and become actual drugs are vanishingly rare. A 3% success rate is the brutal reality of this biological lottery. This explains why novel drugs are so expensive — the cost of one successful drug includes the accumulated costs of all the failed attempts. Many drugs are priced at astronomical levels, say $1 million per course of treatment, for exactly this reason.
(Feel free to share to your Moments. For republication on other official accounts, websites, or mobile apps, please reply "reprint" for our republication policy and contact FreeS Fund for authorization. Copyright belongs to FreeS Fund.)

▲ FreeS Report 14: Cosmetics Keep Getting Pricier — Is Your Face Really Worth a Million?
▲ FreeS Report 13: To Understand China's Consumption Upgrade, Look at Japan 40 Years Ago
▲ FreeS Report 10: The Shared Secret of Hit Snacks That Survived Economic Cycles
FreeS Report 9: How Can Sportswear Brands Achieve Brand Upgrade?
FreeS Report 8: Will the Matcha Industry Produce the Next Starbucks?
FreeS Report 7: Four Major Directions for Healthcare Data Entrepreneurship in China
FreeS Research 6: Keep Just Raised Its Fourth Round — What's Left in the Abs and Gym Business?
FreeS Report 5: We've Collected So Much Health Data — How Far Are We From Living Well?
FreeS Report 4: The SaaS Explosion — Opportunities, Logic, and Challenges
FreeS Report 3: Is an Online IKEA Possible? — Investment Analysis of Home E-commerce
FreeS Report 2: Healthcare Investment Outlook in China and the US
▲ FreeS Report 1: Opportunities and Future of Cross-border E-commerce Exports
