Riding the Gene Therapy Wave | Frees Fund

From Willow Bark to "God's Scalpel" — A Brief History of Drug Development
The "He Jiankui affair" that erupted at the end of 2018 brought gene editing — one strategy within gene therapy — into the public eye.
Since the discovery of DNA's double helix structure in 1953, our understanding of genetics has reached the molecular level. Treating diseases at the genetic level has long been a dream of scientists. After the frenzy and subsequent downturn of the 1990s, humanity finally welcomed its first approved gene therapy drug, Glybera, in 2012. From that point on, the door to gene therapy was thrown open.
From small molecules to protein drugs, nucleic acid drugs, and now gene therapy — how do these various types of drugs actually work? What distinguishes them, and what are their respective characteristics?
Why is gene therapy so powerful yet so controversial? For the first time, humans have the ability to rewrite the genetic code. Is this Aladdin's lamp, or Pandora's box?
In this article, we start from a brief history of drug development and how different drug types interact with the human body, to understand the foundations, current state, and future of gene therapy.
This article will address the following questions in turn:
-
A brief history of drug development: from small molecules to gene therapy 1.1 How each drug type is grounded in its corresponding scientific discipline 1.2 The size and complexity of different drugs
-
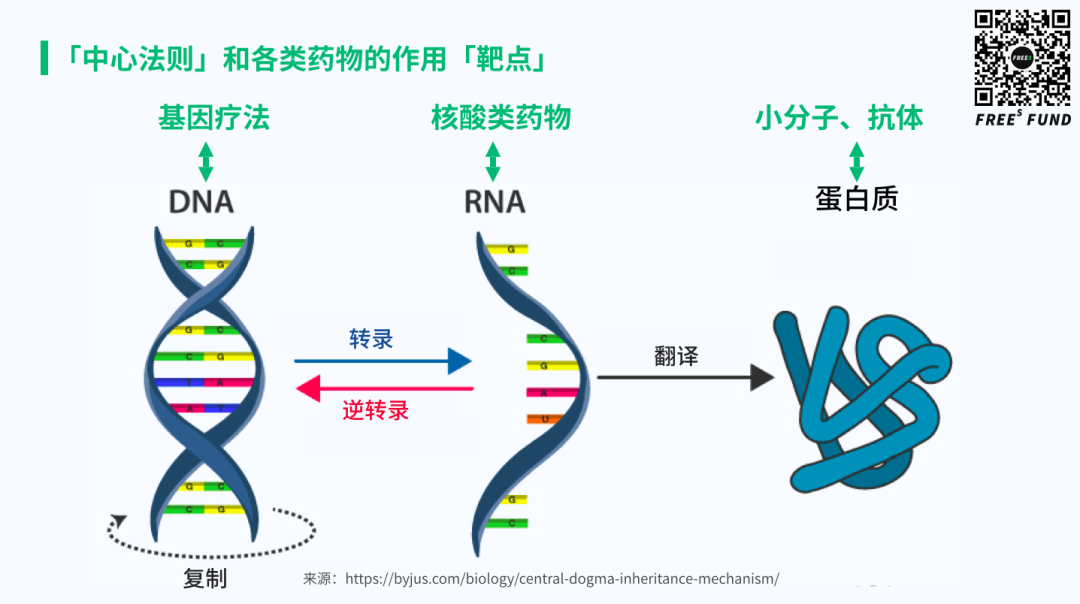
Mechanisms of action for various drug types 2.1 The "central dogma" and two fundamental biological processes 2.2 Different drugs act on different "targets"
-
How powerful is gene therapy? 3.1 SMA — a battlefield where many compete, each showing their strengths 3.2 From rare diseases to common diseases, from treatment to prevention, from health to enhancement
As always, before diving in, here are three key takeaways:
- Drug development has progressed from small molecules and protein drugs to nucleic acid drugs, and has now entered the era of gene therapy.
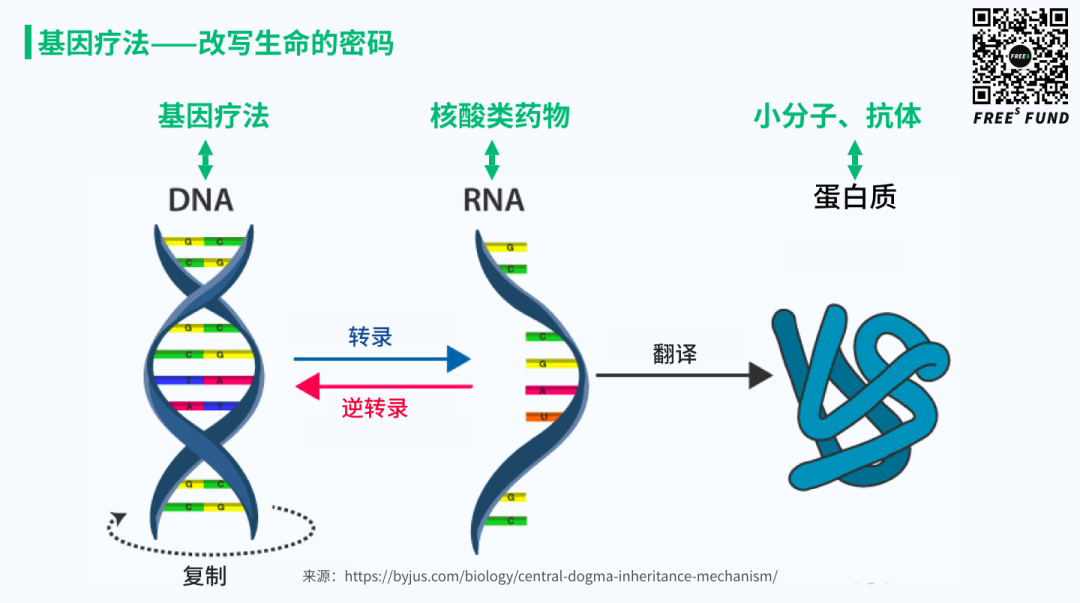
- The "targets" of small molecules, short peptides, and antibody drugs are proteins — they modulate protein function. The "targets" of nucleic acid drugs are mRNA — they modulate protein expression. The "targets" of gene therapy drugs are DNA — they can not only alter protein expression but even heritably modify the protein-coding sequence itself.
- Gene therapy began with rare diseases that have strong causal relationships, and will gradually expand into the treatment and management of common, multi-factorial diseases.
We hope this offers fresh perspective. FreeS Fund continues to pay close attention to innovation in the gene therapy space, and we look forward to exchanging ideas with entrepreneurial teams, practitioners, and industry experts. Feel free to reach out to Yikai Wang at yikai@freesvc.com. Also follow us for our gene therapy forum in Beijing on June 20 (next Saturday) — scan the QR code in the image below to register.


01
Advances in life science research and biotechnology have made the development of increasingly complex drugs a reality
The development of chemistry, molecular biology, and genetics, and the successive emergence of various drug types
- Chemistry and small-molecule drugs
In June 2019, archaeologists discovered high concentrations of tetrahydrocannabinol (THC) residue at a 2,500-year-old burial site on the Pamir Plateau. THC is the primary psychoactive compound in cannabis, producing euphoria and pain relief — the earliest direct evidence of human cannabis use.
Beyond cannabis, over thousands of years of battling disease, people found that many plants had specific therapeutic effects: cinchona bark for malaria, willow bark for fever and colds. These were the precursors of "small"-molecule drugs. With the rise of natural science, by the late 18th century people could already isolate certain components from bark for better results. It wasn't until the early 19th century, when understanding of matter advanced to the molecular and atomic level, that chemistry was born as a discipline — and with it, the era of small-molecule drugs.
- Molecular biology and macromolecular drugs (antibodies), nucleic acid drugs
In the late 18th century, Edward Jenner's cowpox vaccination against smallpox formally established immunology as a discipline. In 1890, Behring and Kitasato discovered antibodies while immunizing animals with diphtheria exotoxin. The 1953 discovery of DNA's double helix structure brought understanding of life to the molecular level. By the 1970s, with the maturation of electron microscopy and genetic recombination technology, molecular biology advanced tremendously. In 1975, Köhler and Milstein invented hybridoma technology, enabling scalable discovery of therapeutic monoclonal antibodies. The first monoclonal antibody was approved in 1997, ushering in the era of macromolecular (antibody) drugs. With the emergence of antisense oligonucleotide and RNA interference technologies, nucleic acid drugs also took the stage.
- Genetics and gene therapy
From Swiss physician Friedrich Miescher's first discovery of nucleic acids in 1868, to Wilkins and Franklin's X-ray diffraction analysis of DNA crystals in the early 1950s, to Watson and Crick's discovery of the double helix structure and proposal of molecular biology's "central dogma," to the development of genetic recombination engineering and viral vectors in the 1970s and 1980s — human understanding and research of genes deepened continuously, and the technical framework for gene therapy gradually took shape.
In 1972, renowned American biologist Theodore Friedmann and colleagues published a landmark forward-looking commentary in Science titled "Gene Therapy for Human Genetic Disease?" — raising the question of whether gene therapy could be applied to human disease.
From the first gene therapy clinical trial in 1990 for severe combined immunodeficiency (SCID), to the 1999 death of 18-year-old Jesse Gelsinger from multi-organ failure during a gene therapy trial at the University of Pennsylvania — the "soap bubble of hope" for gene therapy burst, and the field entered its darkest and most difficult period.
After more than two decades of persistent exploration, gene therapy finally welcomed its second spring. In 2012, Glybera from Dutch company UniQure was approved by the EU, using adeno-associated virus (AAV) as a vector to treat severe muscle disease caused by lipoprotein lipase deficiency. As the first formally approved gene therapy drug, Glybera's success opened a new era for gene therapy.
The size and complexity of different drugs — an analogy with vehicles
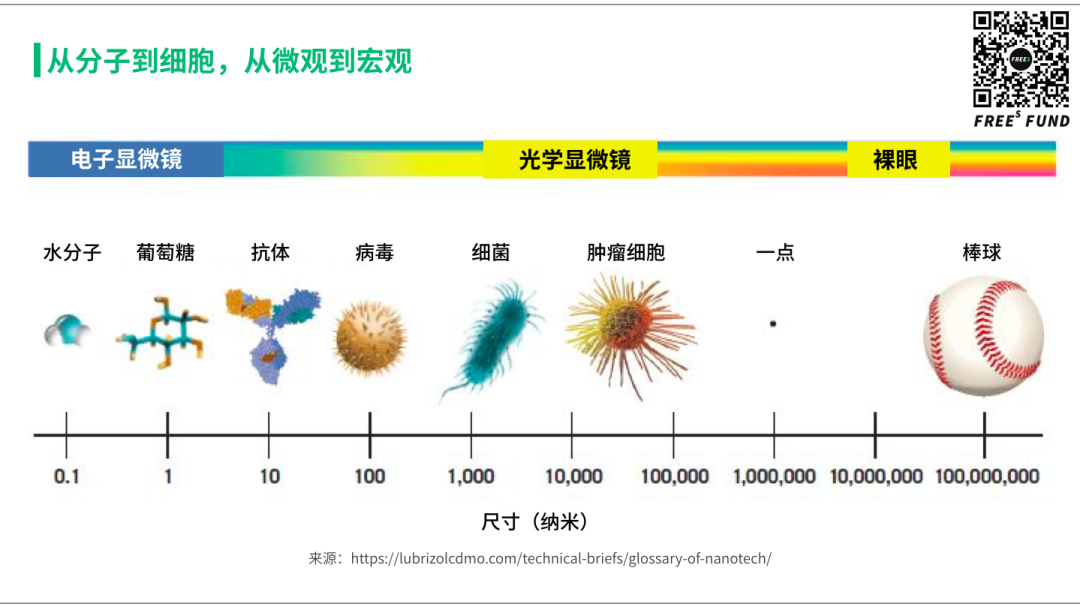
If we arrange molecules to cells by size, the leftmost are small molecules, roughly in the range of a few nanometers. Macromolecular drugs are 1-2 orders of magnitude larger, around 20 nanometers. The most widely used vector in gene therapy today, adeno-associated virus, is roughly comparable in size to antibodies. Other viral vectors are generally larger, reaching around 100 nanometers. Compared to our body's eukaryotic cells, these are still 2-3 orders of magnitude smaller. All of this remains at the microscopic level, requiring microscopes to observe and study. At the level visible to the naked eye — say, a dot we can see — that's already about 100 times larger than a cell.

Let's use vehicles as an analogy to understand the characteristics of different drugs. Small-molecule drugs are like bicycles — easiest to manufacture and produce. Short peptides and small nucleic acid drugs are like cars: considerably heavier and more complex. Macromolecular (antibody) drugs are like airplanes, while viral vectors used in gene therapy are like rockets.
Generally speaking, smaller things are less complex in themselves — that's easy to understand. But when it comes to mechanism of action and functionality, the picture becomes more nuanced.
First, every drug has its appropriate scenario. Continuing the vehicle analogy: if we're visiting relatives nearby, a bicycle is probably the most convenient option. Driving works too, if parking isn't a hassle. But taking a plane or rocket would be absurd.
Second, different drug types have different mechanisms and flexibility. Riding a bicycle to run errands, you might have several destinations and can adjust flexibly — if you change your mind or it suddenly rains, you just head home. But with planes and rockets, the destination is very specific; once launched, it can't be changed except by returning or making an emergency landing — both major events.
Finally, structurally simpler small molecules are actually less safe than antibodies and gene therapy. We might feel that flying is unsafe, but in reality airplanes have the lowest accident rate — they're the safest. Bicycles, by contrast, might actually be the least safe.
The point of this analogy is that every drug has its own characteristics and appropriate applications. The emergence of macromolecular antibody drugs and now gene therapy doesn't mean small-molecule drugs have lost their value or can be replaced. Gene therapy, despite all the buzz, cannot replace antibody or small-molecule drugs either. It is simply a new therapeutic modality that can indeed solve problems that small-molecule and antibody drugs struggle with — just as only rockets can carry us beyond Earth to explore the vastness of space. This is what we'll discuss next.
02
Understanding the mechanisms of different drugs through the "central dogma" and life's two fundamental processes
The "central dogma" and two fundamental biological processes
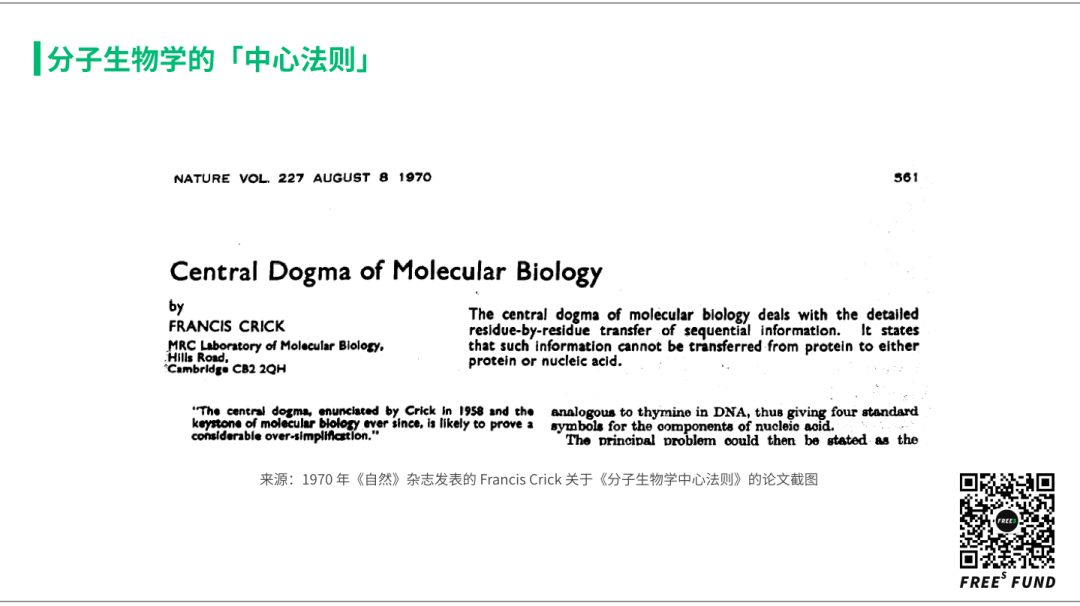
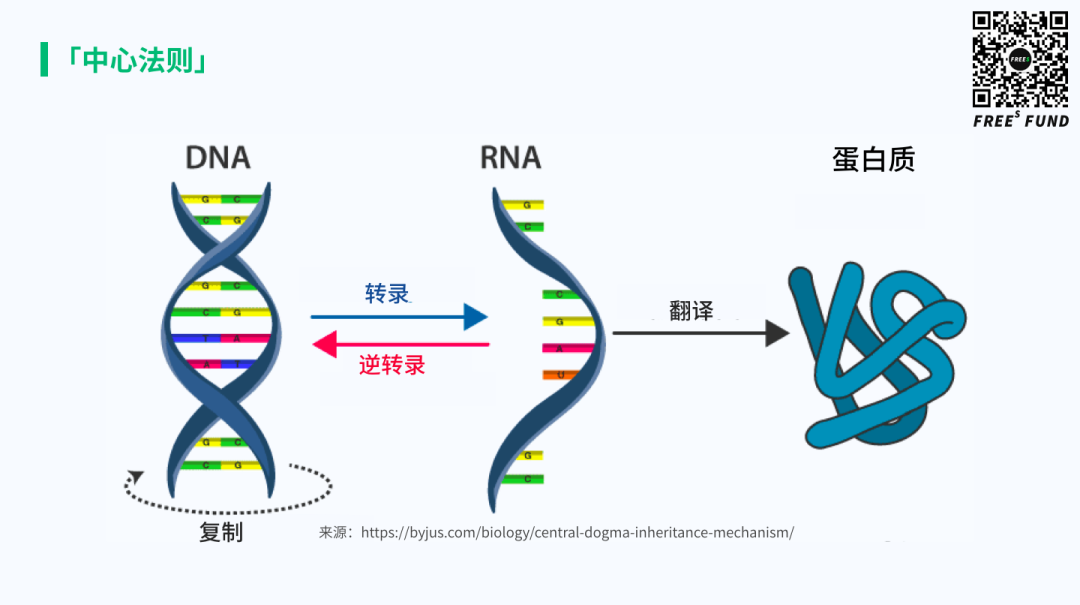
To understand this, let's revisit a foundational concept in modern biology — the "central dogma." Francis Crick proposed it in 1958, and in 1970 he published an article in Nature that distilled its core idea into a single, rather convoluted sentence: "The central dogma of molecular biology deals with the detailed residue-by-residue transfer of sequential information. It states that such information cannot be transferred from protein to either protein or nucleic acid." What this really means, in plain terms, is answering the question: how is genetic information transmitted?
Crick explained that among the three major classes of biological macromolecules — DNA, RNA, and proteins — there are nine possible directions of information flow. These fall into three categories: three general transfers (occurring in most cells), three special transfers (occurring only under specific conditions), and three unknown transfers (presumed not to happen).

Simplified into the familiar diagram below, the central dogma captures one of life's fundamental characteristics: heredity. This is what allows life to persist with stability.
Life is extraordinarily complex. Translation and modification of genetic information underpin countless biological processes within organisms. Here, we'll focus on two particularly important ones: signal transduction and metabolism.
Signal transduction addresses how life perceives and regulates signals — both from the outside world and within itself. From the moment a fertilized egg begins to divide, through differentiation and development, through sensing and responding to external stimuli, self-protection, and in higher animals, through memory, emotion, and eventually aging — all of these involve signal transduction and regulation. Over hundreds of millions of years of evolution, nature has crafted remarkably complex yet precise regulatory systems, enabling life to exist in its present forms and allowing humans to emerge as a species.
Metabolism addresses the exchange of matter and energy between an organism and its environment. Life is an open system; to maintain normal function, it must continuously take in substances and expel waste, solving problems of energy production, storage, and utilization.
You may have noticed some relatively simple structures or nodes in these processes — these are small molecules. The material foundation of life is built from small molecules, from the simplest like oxygen and carbon dioxide to sugars, amino acids, and lipids. The transformations between these substances involve vast numbers of enzymes (a class of proteins that catalyze chemical reactions). The mechanisms by which these enzymes interact with small molecules constitute the main subject matter of what we call biochemistry.
Different drugs act on different "targets"
First, the origins of disease. Some diseases have relatively simple causes, such as monogenic inherited disorders; others are more complex, like cancer or metabolic diseases.
Second, the purpose of drugs is to correct these problems and defects, with the precondition of minimally disrupting normal biological activity — otherwise side effects may occur. If a drug's benefits don't outweigh its side effects, we say in technical terms that its therapeutic window is too narrow; in plain language, the drug does more harm than good and has limited value.
- Small molecules, short peptides, and large-molecule antibody drugs: targeting proteins
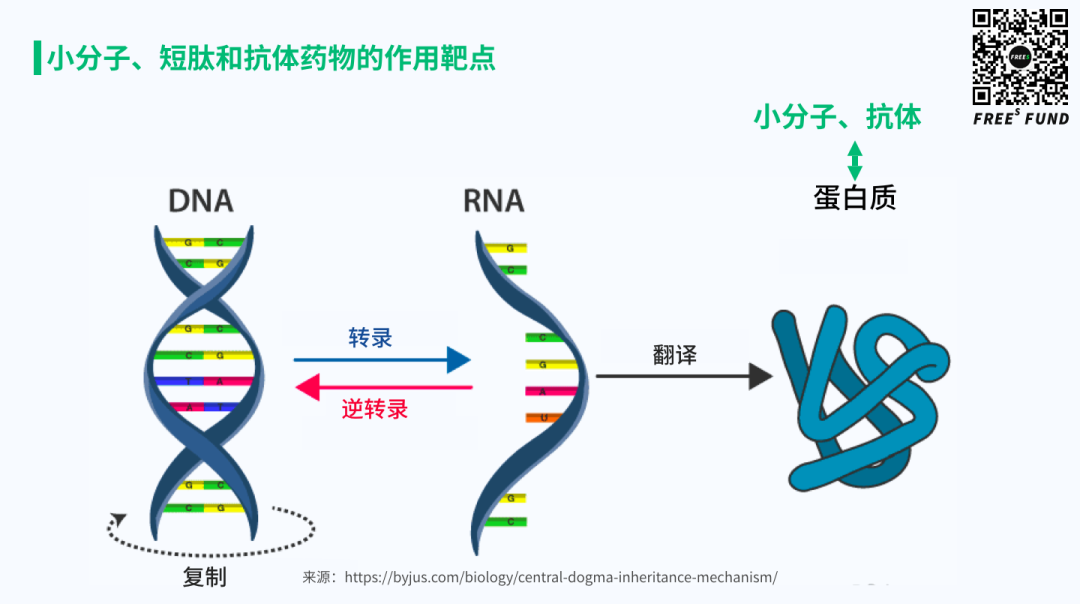
Small molecules, short peptides, and large-molecule antibody drugs generally work through proteins. We say their "targets" are proteins. The two major functions mentioned earlier — signal transduction and metabolism — are primarily carried out by proteins. So broadly speaking, these drugs treat disease by influencing protein function to intervene in signal transduction, metabolism, and other processes. We collectively refer to these as targeted therapies.
But if they all target proteins, what's the difference between small molecules and peptide/antibody drugs?
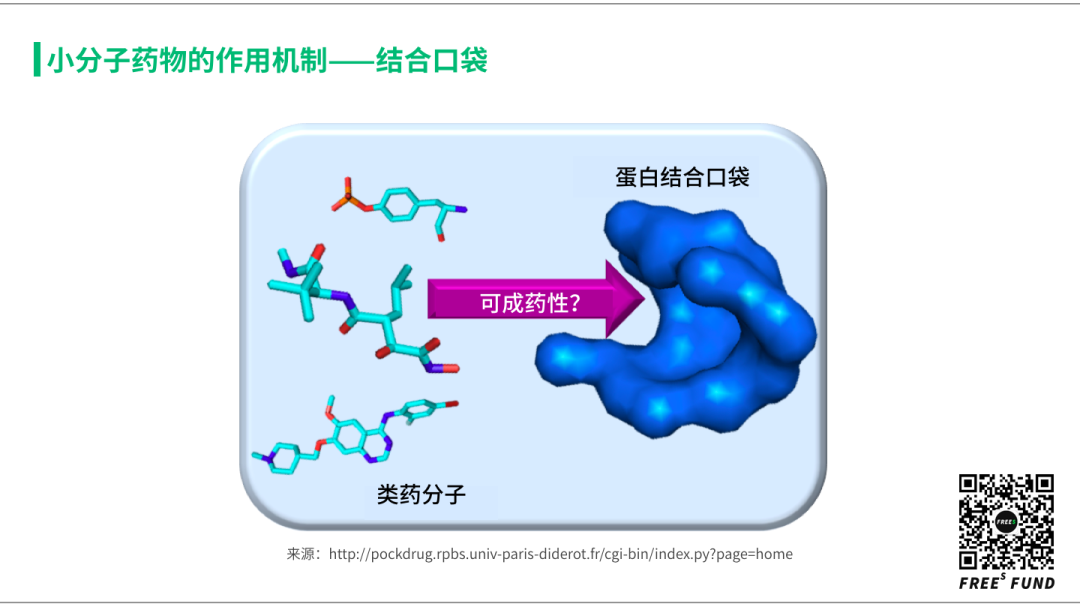
First, because small molecules can freely cross cell membranes, their targets can be located inside cells. Antibodies and short peptides, however, mainly act on membrane proteins or extracellular proteins.
Second, the protein targets of small molecules are typically those that normally interact with naturally occurring small molecules in the body — such as metabolic enzymes with metabolites, GPCRs with small-molecule signaling molecules, and kinases with small-molecule cofactors. Antibody targets, by contrast, usually involve ligand-receptor interactions, commonly known as protein-protein interactions.
Considering the origins of these two drug classes helps explain their differences. The earliest bioactive small molecules — such as the previously mentioned tetrahydrocannabinol, quinine, and aspirin — were originally metabolic products of various species. These molecules were synthesized by proteins to bind other proteins (sometimes in other species), conferring evolutionary advantages. It just so happened that in humans, we discovered their therapeutic effects and acceptable therapeutic windows, leading to their development as drugs.
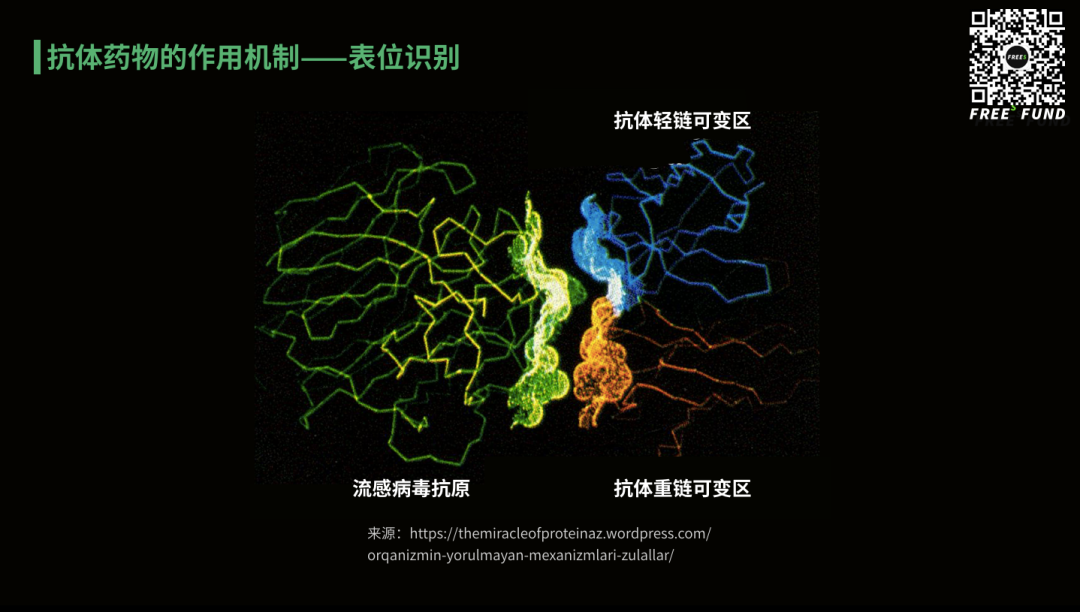
As mentioned earlier, antibodies are weapons the immune system uses to resist foreign invasion and a mechanism for the body to inspect and correct itself. Because proteins exposed on cell surfaces (including bacteria and viruses) are the most effective markers for distinguishing self from non-self and normal from abnormal, the immune system uses antibodies to recognize and differentiate between the body's own normal proteins and invading, abnormal ones — distinguishing "self" from "non-self." Thus, the main targets of antibody drugs are membrane proteins and extracellular proteins, and their primary recognition mode is so-called protein-protein interaction, also known as "epitope recognition." This is the foundation of immunology and of antibody drugs.
The human body contains roughly 19,000 different proteins; about 5,000 of these (roughly one-quarter) have been found to be disease-related. Among these, approved drugs currently target approximately 700, with roughly 1,200 more considered potentially druggable. Another 3,000-plus disease-related proteins are classified as "undruggable."
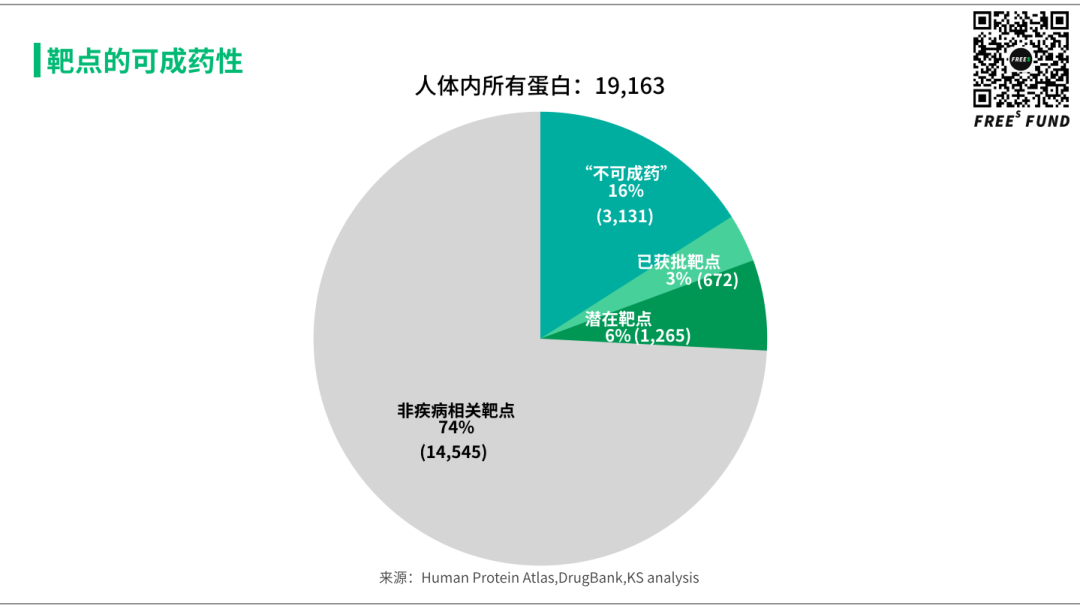
These proteins are mainly located inside cells, inaccessible to antibodies; and no known naturally occurring small molecules interact with them, making small-molecule drug development difficult as well. Of course, the quotation marks around "undruggable" mean this is only true for now. As technical capabilities in small-molecule and antibody fields advance, we are gaining more tools and methods to intervene against these targets — hopefully rendering this definition obsolete, or at least shrinking the number of "undruggable" targets.
- Nucleic acid drugs: targeting RNA
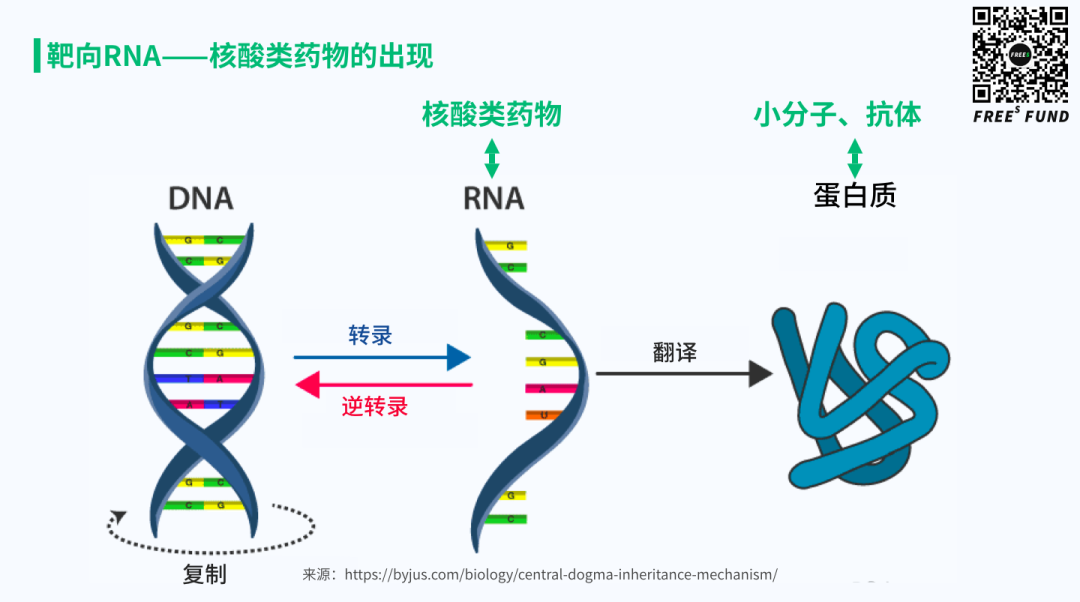
Returning to the central dogma: we've discussed how small-molecule and antibody drugs target proteins. Drugs that target RNA are called nucleic acid drugs. These became possible thanks to two foundational technological breakthroughs: in 1978, Zamecnik and Stephenson discovered antisense oligonucleotides (ASOs), and in 1998, Fire and Mello discovered what became known as RNA interference.
Interestingly, the first ASO paper was published in 1978, and the first ASO drug was approved 20 years later in 1998. Similarly, RNA interference was discovered in 1998, and the first RNAi drug was approved 20 years later in 2018. Roughly two decades — that's how long it takes for a technology to move from discovery to successful clinical application. This milestone extended our systematic ability to regulate life to the RNA level for the first time.
When small-molecule and antibody drugs bind to proteins, they affect certain protein functions — such as signal transduction or catalytic activity — to produce therapeutic effects. However, this functional modulation typically doesn't directly change the concentration of the protein itself (reality is more complex with exceptions; this is a broad simplification). Nucleic acid drugs work through a fundamentally different mechanism: they alter protein expression levels (or expression forms) themselves.
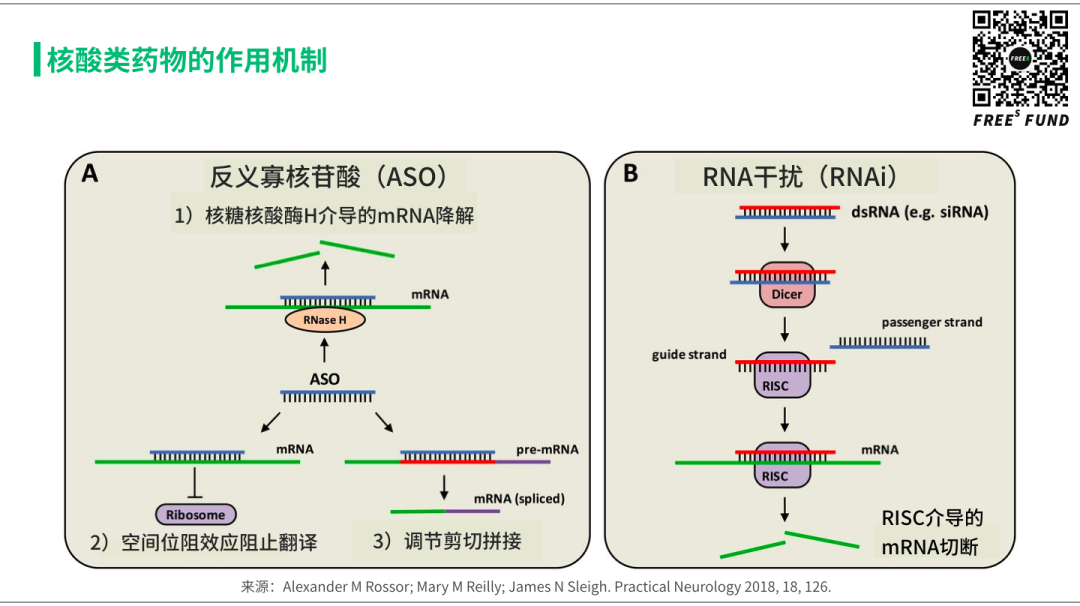
Simply put, whether single-stranded DNA or RNA (ASOs) or double-stranded dsRNA (RNAi), once they bind to their target mRNA, they either directly degrade the mRNA, block its translation into protein, or affect its splicing to produce different protein forms. In any case, the expression level (or form) of the protein is changed — this is the mechanism of nucleic acid drugs.
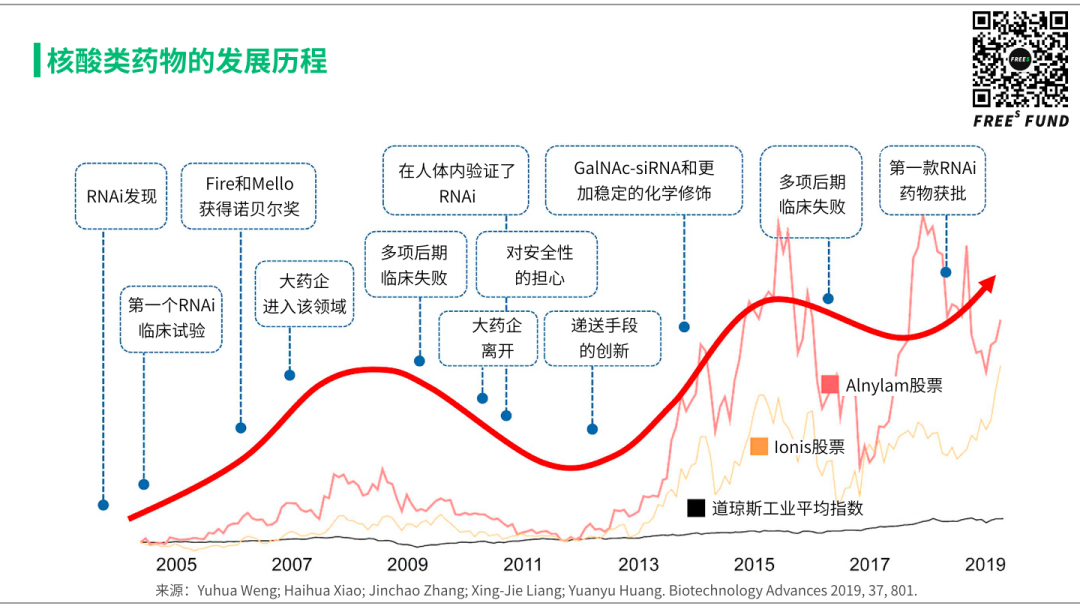
Looking at the history of nucleic acid drugs, two representative companies in this space have ridden multiple boom-and-bust cycles — at least two full Hype Cycles, you could say.
The first was the validation of RNA-targeting technology itself in the human body. The second was a breakthrough in delivery methods that finally opened up a viable therapeutic window in the clinic. The recent approval of several blockbuster drugs in particular has sent platform companies built on this technology into favor with both industry and investors. Interested readers can look up the relevant coverage and review articles.
Here, let's return to comparing the characteristics and differences of various drug modalities, using that contrast to understand the promise and limitations of nucleic acid drugs.
As mentioned earlier, the first ASO drug, Fomivirsen, was approved in 1998 as a second-line treatment for cytomegalovirus (CMV) retinitis. But with the advent of highly active antiretroviral therapy, CMV cases plummeted — and the drug was withdrawn from Europe in 2002 and the US in 2006.
This outcome was hardly surprising. Antiviral applications have always been small molecules' strong suit. That hasn't stopped continued exploration of nucleic acid drugs in antiviral settings, though — from SARS in 2003 to COVID-19 this time around, scientists have studied using this technology to suppress viruses. But that's a story for another day.
Another well-known RNAi drug, Bevasiranib, targeted VEGF mRNA to treat age-related macular degeneration (AMD). It completed Phase 3 trials in 2008, only to have development halted in 2009.
Why? Because VEGF is a growth factor — it binds to its receptor VEGFR to promote angiogenesis — and the optimal modality for blocking this interaction is antibodies. In 2006, Genentech's Lucentis won approval and quickly became the gold standard. Bevasiranib quietly exited the stage.
2018 was a watershed year for nucleic acid drugs. The FDA approved two nucleic acid therapies for hereditary transthyretin amyloidosis (hATTR) in quick succession: Tegsedi, an ASO developed by Ionis, and Onpattro, from Alnylam — the first approved RNAi drug.
hATTR is a rare, progressive, systemic, fatal hereditary neurological disease caused by abnormal formation and aggregation of TTR amyloid protein that deposits in organs and tissues throughout the body.
Both Tegsedi and Onpattro dramatically reduce TTR protein levels and deliver meaningful improvements in neuropathy and quality of life. The two drugs were expected to face off fiercely on pricing, convenience, real-world efficacy, and marketing. But regardless of the outcome, their approvals brought enormous enthusiasm and hope to the industry — because this is exactly the kind of application where nucleic acid drugs shine.
In terms of problems they can solve, nucleic acid drugs have distinct strengths compared to small molecules and antibodies. But from a drug development perspective, they must clear far more hurdles to actually work — far more than small molecules or antibodies.
First, unlike small molecules and antibodies, nucleic acid drugs have poor stability in blood and issues with immunogenicity.
Second, nucleic acid drugs carry multiple negative charges on their surface and cannot cross cell membranes on their own. Yet their targets are mRNA molecules, meaning they must enter the cytoplasm to function. Intracellular delivery is thus a massive challenge.
Finally, large-scale manufacturing and quality control for nucleic acid drugs is more complex than for antibodies, and vastly more complex than for small molecules — limiting large-scale R&D and exploration. This explains why nucleic acid drug development went through multiple Hype Cycles before reaching its current level.
- The New Frontier: mRNA as Drug
After the COVID-19 pandemic, mRNA vaccines and Moderna need no introduction. As the highest-market-cap unicorn IPO in US biotech history, Moderna's origin story is legendary and fascinating — well worth reading up on. The nucleic acid drug companies mentioned earlier used mRNA as a target, but in recent years a wave of companies including Moderna have chosen to use mRNA itself as the therapeutic.
Moderna had already been developing mRNA vaccines against CMV and influenza; the pandemic simply threw a sudden spotlight on this direction, even though no mRNA vaccine had yet been approved for infectious disease prevention. For COVID-19 specifically, Moderna skipped preclinical animal validation and went straight to human administration. We'll set aside ethical questions and ultimate efficacy for now — for Moderna, this was a commercial success, and for the entire mRNA field, a rare boost in visibility.
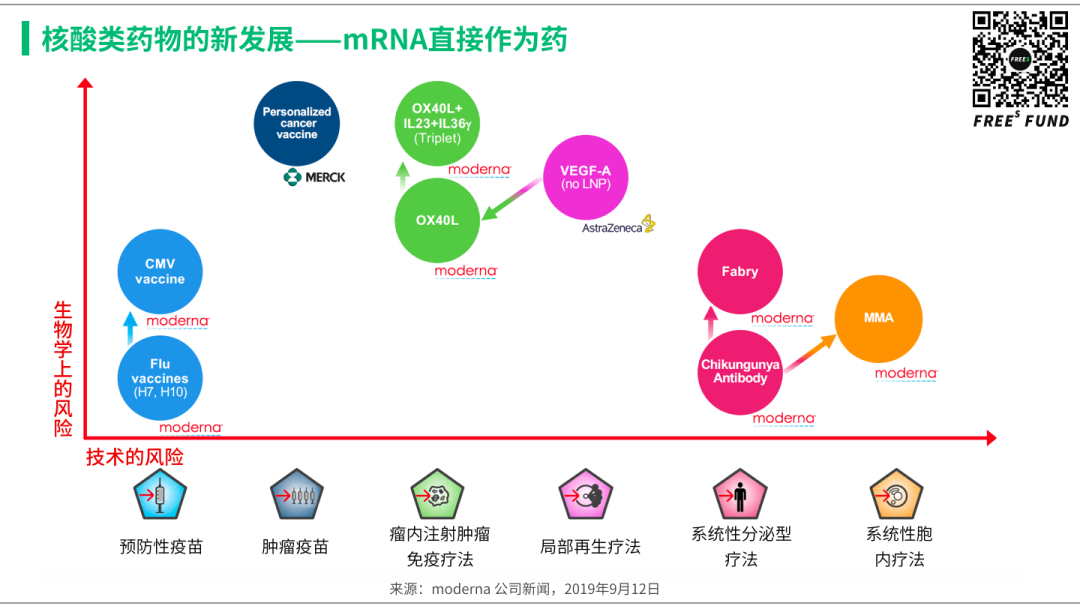
On Moderna's pipeline, a few more words. Take a look at this chart, from an investor relations presentation last year. The strategic thinking behind this pipeline layout is quite interesting, and worth studying for anyone developing novel therapeutic modalities.
The y-axis is "biological risk," the x-axis "technical risk." In plain terms: the higher up the y-axis, the more uncertain the biological causality — whether it can actually treat the disease is unclear, hence higher risk. The further right on the x-axis, the more technically difficult to implement, the more problems to solve, the greater the challenges, and again the higher the risk.
How did Moderna arrange its own pipeline?
First, it obviously chose directions with low risk on both dimensions: prophylactic vaccines for CMV, influenza, and COVID-19.
Second, it selected genetic diseases where the technical challenges are substantial but the biological causality is strong. The logic: with clear biological mechanisms, if clinical results disappoint, you only need to solve technical problems — and technical problems are relatively easier to explain, iterate, and improve.
Finally, there are directions with large technical risk (though perhaps not the largest) but especially high biological uncertainty, such as cancer vaccines and cytokine therapies related to tumor immunity.
Compared to the therapeutic areas mentioned earlier, breakthroughs here would mean enormous markets and handsome returns — but they carry uncertainty and risk on both fronts. So Moderna chose to co-develop with large pharma, sharing risks and rewards. Moderna's rise to become the most successful unicorn in history offers plenty to learn from, from technical moats to strategic direction.
This introduces two concepts — "biological risk" and "technical risk" — that provide a crucial analytical framework for the gene therapy discussion to follow.
- Gene Therapy: DNA as "Target"
Let's return to the "central dogma." Ever since DNA was discovered as the core carrier of our genetic information, attempts to alter it have never stopped.

Speaking of gene therapy, one cannot skip James Wilson. On September 17, 1999, Jesse Gelsinger received a high dose of adenovirus (Ad) carrying a corrective gene in James Wilson's lab at the University of Pennsylvania, to treat the rare metabolic liver disease ornithine transcarbamylase deficiency. Four days after treatment, Jesse died from a massive immune response causing multi-organ failure and brain death. James was stripped of his title, his gene therapy center was disbanded, and he was banned from conducting any clinical trials until 2010.
James downsized his lab and focused on finding safer viruses. His team's work led to the discovery and dissemination of novel adeno-associated viruses (AAV), including AAV9 used in the recently approved gene therapy Zolgensma.
On September 17, 2015 — the 16th anniversary of Jesse's death — Regenxbio, a biotech company built on new AAV vectors, went public on Nasdaq. According to the latest University of Pennsylvania statistics, approximately 42 companies are using AAV covered by Wilson's patents, spanning nearly 100 drug development programs. Gene therapy went from nadir to peak, and James witnessed it all.
Returning to our analytical framework: gene therapy's greatest technical risk lies in drug delivery. The requirements exceed even those for nucleic acid drugs — gene therapies must reach the nucleus to work, since genes themselves reside there. Thus early and current gene therapies have predominantly used viruses as delivery vehicles. The 1999 tragedy with Jesse was directly linked to the use of adenovirus as a vector. As we've analyzed, delivery and manufacturing are already major challenges for nucleic acid drugs — to say nothing of using infectious live viruses as vectors.
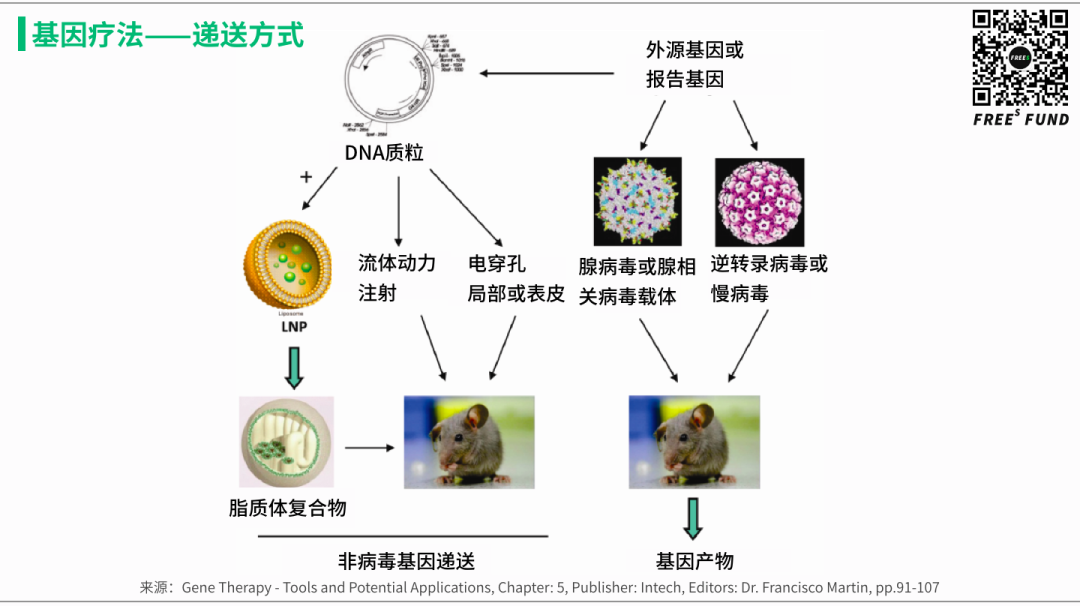
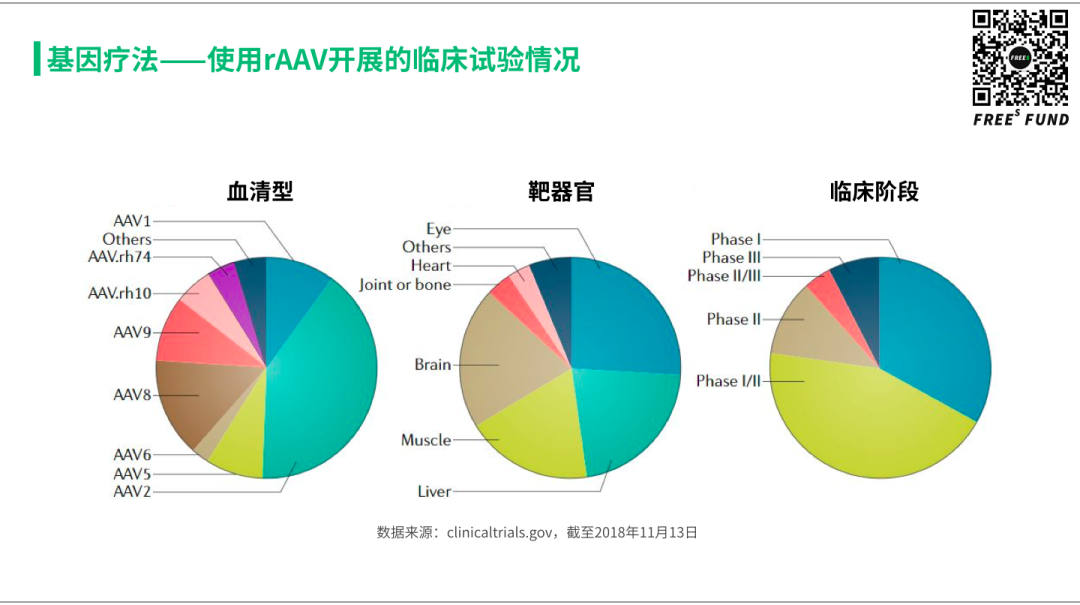
Fortunately, researchers soon discovered that adeno-associated virus (AAV) could serve as an ideal delivery vehicle — efficiently transporting therapeutic payloads into the cell nucleus while remaining safe and controllable, with relatively low risk and side effects to the human body. By the end of 2018, approximately 145 clinical trials using AAV for gene therapy were underway, targeting primarily the eyes, muscles, liver, and nervous system. Naturally, the vast majority of indications were genetic or rare diseases caused by single-gene abnormalities. But as technical risks and uncertainties gradually diminish, gene therapy will quickly expand into common diseases like AMD and Parkinson's.
Gene therapy can be broadly categorized into four approaches: gene replacement, gene addition, gene silencing, and gene editing.
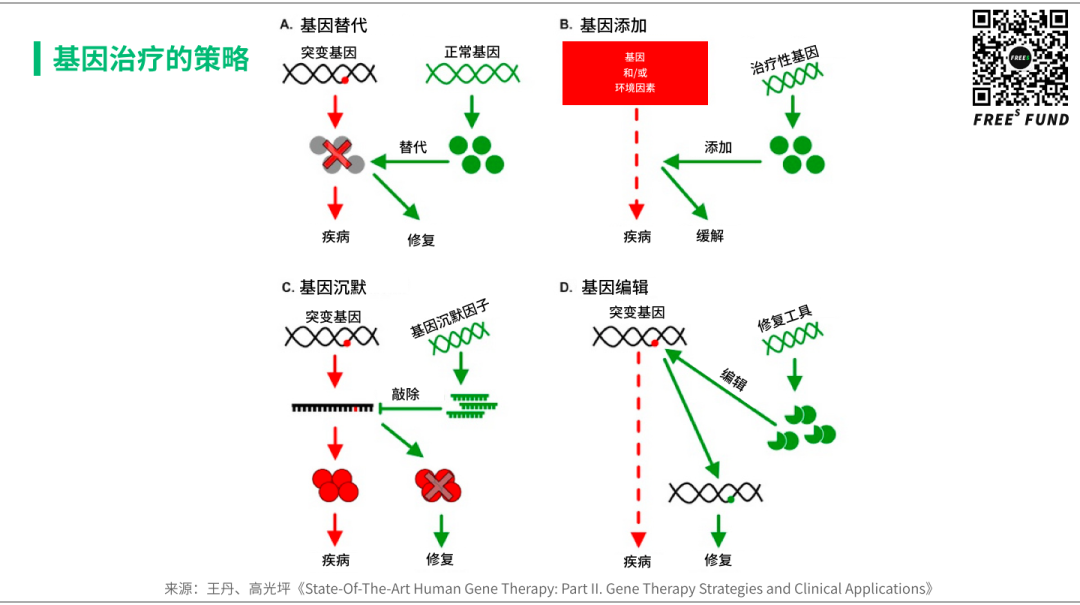
- Gene replacement
This strategy aims to provide a gene product to compensate for loss-of-function mutations. Gene replacement is suitable for treating recessive monogenic diseases and has achieved the greatest clinical success to date, as evidenced by approved therapies like Glybera and Luxturna.
- Gene addition
Beyond monogenic diseases, rAAV-mediated gene therapy may also address complex genetic and acquired conditions through gene addition — such as heart failure and infectious diseases. Additionally, rAAV can be used to deliver antibodies: once muscle cells are transduced, they can effectively become biological factories, producing therapeutic antibodies and secreting them into the bloodstream.
- Gene silencing
In contrast to gene replacement, gene silencing primarily addresses monogenic diseases caused by gain-of-function mutations. Currently, this is achieved using rAAV to deliver RNAi. However, compared to nucleic acid drugs (siRNA and ASO), rAAV-based RNAi therapies remain largely in preclinical development. Recently, uniQure's AMT-031 IND application for Huntington's disease received FDA approval.
- Gene editing
rAAV can be used to deliver CRISPR-associated (Cas) proteins to directly repair disease-causing mutations in humans.
For specific progress in gene therapy, interested readers can consult relevant reports or reviews. Here, we'll use two examples to understand the characteristics, limitations, and prospects of gene therapy — and why it has sparked such widespread societal attention and debate.
/ 03 / How Powerful Is Gene Therapy?
With "God's Scalpel" in hand,
can we now intervene in heredity itself — this fundamental law of nature?
▍SMA — A Crowded Field, Each Contender Showing Its Strengths
SMA is a rare inherited neuromuscular disease. Due to the lack of a functional SMN1 gene, SMA causes rapid and irreversible loss of motor neurons, affecting muscle function including breathing, swallowing, and basic movement. SMA is the leading genetic cause of death in infants under two years old, with Type 1 SMA being the most common form, accounting for approximately 60% of all cases. Without treatment, over 90% of patients die or require permanent ventilation by age two.
At the end of 2016, the FDA approved Spinraza, the first SMA treatment drug developed by Ionis. Spinraza is an antisense oligonucleotide (ASO) administered via intrathecal injection, delivering the drug directly into the cerebrospinal fluid (CSF) surrounding the spinal cord. Spinraza aims to alter the splicing of SMN2 pre-mRNA to increase production of full-length, functional SMN protein — levels of which are insufficient in SMA patients, leading to degeneration of spinal motor neurons. In clinical studies, Spinraza treatment significantly improved motor function in SMA patients.
In May 2019, Zolgensma — using AAV9 as a vector developed by James Wilson's group — received FDA approval, becoming the world's first gene therapy for SMA. This one-time gene therapy aims to address the genetic root of SMA by replacing the function of the missing or nonfunctional SMN1 gene. After a single intravenous (IV) infusion, Zolgensma delivers a functional copy of the SMN gene into the patient's cells, enabling sustained expression of SMN protein to halt disease progression and thereby improve long-term quality of life.
Meanwhile, Roche is developing an oral small-molecule drug, Risdiplam, a survival motor neuron 2 (SMN2) splicing modifier for the treatment of all types of SMA. The drug is currently under FDA priority review, with a decision expected soon. If approved, Risdiplam will become the first oral drug to treat all three types of SMA.
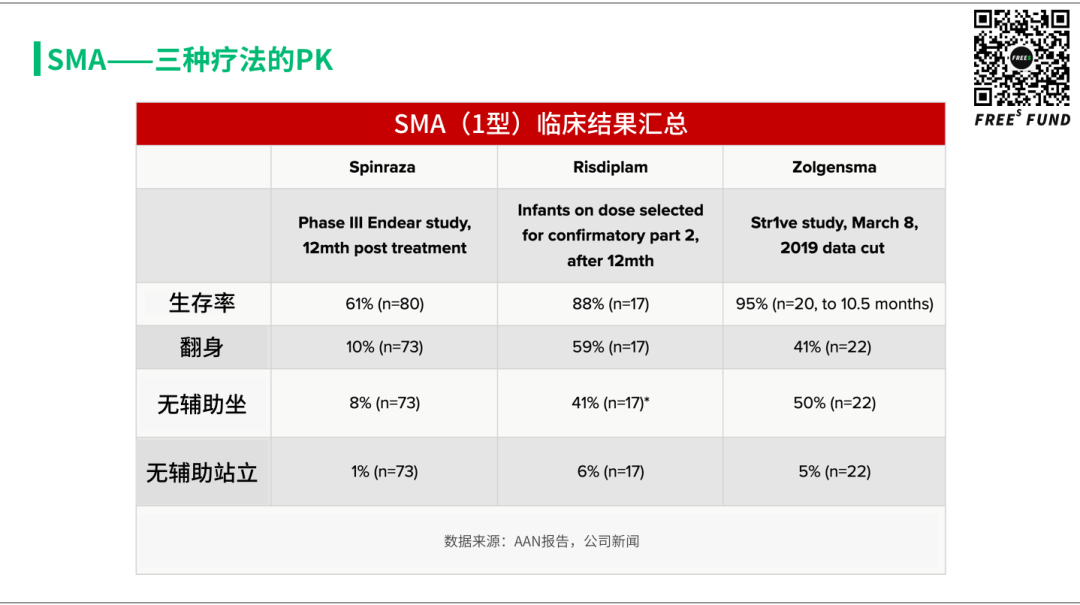
One indication, three drugs: the nucleic acid drug Spinraza, the gene therapy Zolgensma, and the small molecule Risdiplam.
In terms of efficacy, currently published clinical results show that gene therapy appears to have the best survival rate — 95% of patients survive. Looking at improvements in rolling, sitting, and standing among infant patients, small molecules and gene therapy are roughly comparable, both outperforming Spinraza.
From a convenience perspective, Spinraza requires bone marrow puncture to confirm Type 1 genetic mutation before use; Zolgensma doesn't require bone marrow puncture, but patients must be negative for anti-AAV9 antibodies; Risdiplam doesn't require puncture to confirm genotype and applies to all three genetic types — what restrictions it may have for patients remains uncertain.
On pricing: Spinraza costs $750,000 in the first year, then $375,000 annually; Zolgensma requires only a single IV administration, with a price tag of $2.1 million — the most expensive drug in history — payable over five years; Risdiplam requires long-term use, with pricing currently unknown.
For the same indication to simultaneously have three completely different therapeutic approaches is rare in the history of human disease treatment. Equally unexpected was that competition from small molecules emerged in what was supposed to be gene therapy's strongest domain. Regardless of how these drugs fare in the market, they represent the greatest blessing for children with SMA.
It is no exaggeration to say that gene therapy has opened a new door for us — our arsenal of disease interventions has grown richer, and our understanding and conception of health will undergo revolutionary change. At the same time, we face a series of ethical and moral challenges.
▍From Rare Diseases to Common Diseases, From Treatment to Prevention, From Health to Enhancement — Where Are We Headed?
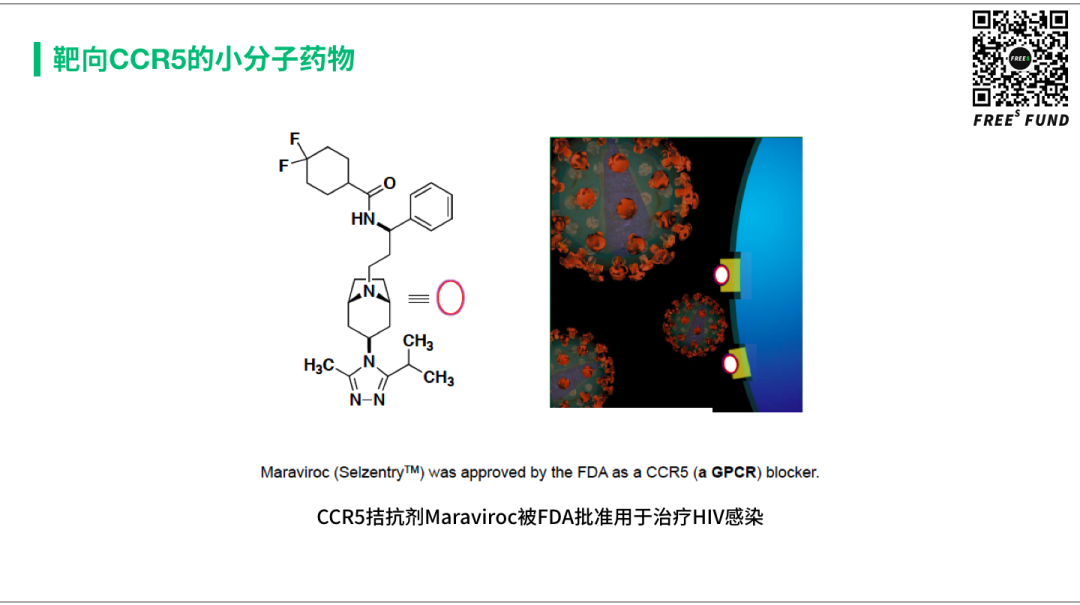
CCR5 is a GPCR found on T cells. For HIV to infect T cells, it must bind to this receptor. The initial discovery of this gene's connection to HIV came from an epidemiological study. This study found that a small subset of high-risk individuals were resistant to HIV infection — and in this group, the gene encoding CCR5 had mutated. Subsequent large-scale population genetic sequencing revealed that in Caucasians, roughly 10-20% of people have half of this gene deleted; approximately 1-2% have the gene completely deleted, and these individuals are virtually completely resistant to HIV infection. Scientists subsequently discovered CCR5's function and its critical role in HIV infection of cells.
CCR5 is a membrane protein that can be blocked with either small molecules or antibodies, both of which can prevent HIV infection. In 2007, Pfizer's small-molecule CCR5 antagonist Maraviroc received FDA approval. This year, CytoDyn's antibody drug leronlimab is expected to gain FDA approval.
While drug development proceeded, the medical community harbored a bold idea: could HIV patients be transplanted with blood from CCR5-deficient donors, thereby achieving a cure? This brings us to the first and second "Berlin patients." Since the first patient was anonymous and information is incomplete, we'll focus mainly on the second.
In 2006, a 40-year-old German Caucasian male named Timothy Brown was admitted to a local hospital and diagnosed with acute myeloid leukemia. This patient had also been diagnosed with HIV ten years prior and had been on antiretroviral therapy. His physician, Gero Hütter, arranged for him to receive a bone marrow transplant from a donor with the CCR5 deletion. If the transplant succeeded, the T cells in this HIV-infected patient would also lack CCR5 — would that make him resistant to HIV?
Fortunately, such a donor was found. Timothy underwent two bone marrow transplants, one in 2007 and another in 2008. Timothy stopped taking antiretroviral drugs on the day of his first transplant. Three months after the first bone marrow transplant, HIV levels in his body rapidly dropped to undetectable levels, while his CD4-T cell count increased. As of 2011, Brown had not resumed antiretroviral therapy. Despite some controversy, Timothy is considered the first person to achieve a functional cure for HIV.

With gene therapy as a new tool, researchers began hoping to replicate the "Berlin Patient's" success. If you could engineer an HIV patient's T cells to silence the CCR5 target, could you cure HIV? A company called American Gene Technologies developed a gene therapy called AGT103. The approach: isolate a patient's T cells, use AGT103 to silence the CCR5 gene, culture the cells ex vivo, then reinfuse them into the patient. Without CCR5 receptors on their T cell surfaces, the patient would no longer be susceptible to HIV infection. Like the Berlin Patient, this would represent a true cure. The therapy is currently in clinical trials.
Where there are bold ideas, even wilder things inevitably follow. That brings us to the He Jiankui affair that erupted at the end of 2018 — editing embryos directly, knocking out the CCR5 gene in the hope that the fetus would never face HIV infection risk. Of course, this ignited massive ethical challenges worldwide.
Wang Liming, a professor at Zhejiang University's Life Sciences Institute, has likened gene editing to "God's Scalpel." I happened to recently rewatch the 1997 Hollywood film Gattaca, which follows Vincent, a "natural" man who never underwent genetic modification, as he assumes the identity of Jerome, a genetically superior man who is unexpectedly paralyzed, to pursue his dream of space travel.
If the He Jiankui affair was only the beginning, and with "God's Scalpel" in hand we could make a wish to make ourselves and our descendants more beautiful, more intelligent, more long-lived — for our species, would this be a dream-come-true Aladdin's lamp, or an uncontrollable Pandora's box?
Key Takeaways
1. Drug development has evolved from small molecules and protein drugs to nucleic acid therapies, and has now entered the era of gene therapy.
2. Small molecules, short peptides, and antibody drugs target proteins, modulating their function; nucleic acid drugs target mRNA, regulating protein expression; gene therapies target DNA, capable not only of altering protein expression but even heritably modifying protein-coding sequences.
3. Gene therapy began with rare diseases where causal relationships are strong, and will gradually expand into the treatment and management of multifactorial common diseases.
Discussion Question
Q: In the gene therapy field, which has better prospects — platform companies or product pipeline companies?
Please hit "View" at the end of this article, and reply "基因" in the WeChat official account backend to see our preliminary answer.
Feel free to share your thoughts on gene therapy in the comments. By 9:00 PM on June 16, the six most thoughtful commenters will each receive a copy of The Gene: An Intimate History (《上帝的手术刀-基因编辑简史》) by Professor Wang Liming.
**/ 04 / ** FreeS x YHCC x BioWorld
Gene Therapy: Opportunities and Future Trends Forum
FreeS Fund, in partnership with YHCC (Yale University China Health Council) and BioWorld, will host the Gene Therapy: Opportunities and Future Trends Forum in Beijing on Saturday, June 20, from 1:30 PM to 5:30 PM. We will conduct in-depth discussions on the current state and latest advances in gene therapy, development opportunities, and entrepreneurship/investment opportunities.
Topics we will explore:
-
Why are we standing at an inflection point for gene therapy?
-
What is the current state of the gene therapy industry?
-
What does Gene Therapy 2.0 technology encompass?
-
What entrepreneurial and investment opportunities exist in the gene therapy space?
...
For this event, we have invited the Head of Cross-Boundary R&D China at Boehringer Ingelheim, the Head of External Innovation and Business Development at Pfizer, leaders from rare disease patient organizations, physicians, academics, and professional investors from Sherpa Healthcare Partners, Qiming Venture Partners, Lilly Asia Ventures, and other institutions to discuss these topics together.
We sincerely invite practitioners, scientists, and entrepreneurial teams with ideas in the gene therapy space to participate and exchange insights.
Please scan the QR code below or click "Read More" to register. Registration requires review; only 15 seats available. The specific address will be notified upon approval.
(Welcome to read, share, and hit "View." For reprint permission, please reply "转载" to learn about our reprint policy and contact FreeS Xiaorui [ID: freesfund] for authorization. Copyright belongs to FreeS Fund.)

FreeS Report 16: The Truth About Early-Stage Healthcare Investment and China Speed | Frees Fund
FreeS Report 15: Life's Gamble — The Adventurous Journey of Drug Development | Frees Fund
2020: Consumer Brand Entrepreneurship Enters an Era of Multiple Simultaneous Growth Drivers | Frees Fund Why New Infrastructure Is China's Most Consequential Stimulus Policy for the Next Decade | Li Feng Column One Chart to Understand China's Supply Chain Changes and Opportunities | Li Feng Column
