The Truth About Weight Loss, and Innovation Opportunities | FreeS Fund Report 36

Every unique you deserves a healthier, more vibrant body.
How to scientifically manage body weight is a perennially hot topic. Transformation stories can be inspiring, but any goal should be grounded in science and reason.
In this FreeS Fund report, we examine weight loss through the intersecting lenses of technology, medicine, and consumer trends. We studied authoritative papers, clinical trial reports, and relevant books on weight reduction, distilling the key insights to help you better understand your body and your weight.
Surprisingly, we found that many truths about weight loss defy conventional wisdom:
- Weight loss becomes harder with age. After adulthood, the number of fat cells in our bodies remains essentially stable, but their volume can expand dramatically — a single fat cell can grow up to 1,000 times larger. In this sense, there may be no upper limit to obesity.
- Uncontrolled appetite is one trigger for obesity, yet dieting and exercise actually increase appetite. That said, lifestyle adjustments remain beneficial in the long run, improving both physical and mental health.
- "Miracle" weight-loss drugs mainly work by suppressing appetite and regulating gastric emptying. But they're not for everyone — obesity has different underlying causes, and results vary. Weight tends to gradually rebound after stopping the medication; combining drugs with dietary and exercise adjustments can prolong their effects.
- For severely obese patients, surgery shows the most pronounced and durable results, but safety varies by individual, and there may be long-term negative effects.
For individuals, the journey of losing weight is often long, lonely, and filled with anxiety and confusion. Don't be too hard on yourself — your body weight isn't simply a matter of willpower, since everyone's absorption and metabolic rates differ. While striving to maintain good physical and mental health, we should also embrace diverse standards of beauty. Weight control has never been about seeking others' approval or conforming to a single ideal, but about responding to and protecting our own well-being.
Join the Conversation
What innovation opportunities do you see in the weight loss and weight management market? What weight-loss methods have you tried?
Share your thoughts in the comments. By 17:00 on April 2, 2024, the five most thoughtful commenters will receive a wellness gift pack (including The Story of the Human Body and DGI snacks from Methuselah).

/ 01 / What Is Obesity?
As we age, our basal metabolic rate generally declines, leading to reduced energy expenditure and weight gain. Basal metabolism refers to the rate of energy expenditure while at rest in a neutrally temperate environment, in the post-absorptive state — meaning the digestive system is inactive, and it requires about 12 hours of fasting in humans. If your current weight is somewhat higher than in your youth, perhaps there's no need for excessive worry.
Whether weight intervention is truly necessary depends on answering these questions: From a medical and health perspective, does your weight actually reach the threshold of obesity? And does this state genuinely pose negative health risks?
Obesity has clear medical criteria. The widely accepted measure is BMI (Body Mass Index). BMI equals weight in kilograms divided by height in meters squared. According to WHO standards, a BMI between 24 and 28 indicates overweight, while 28 and above indicates obesity.

However, we shouldn't look at weight alone — body fat percentage matters too. Weight reflects not just fat but also muscle mass; someone with a high BMI might simply be more muscular. Fat is the body's primary energy storage substance and essential for survival; only excessive accumulation leads to obesity.
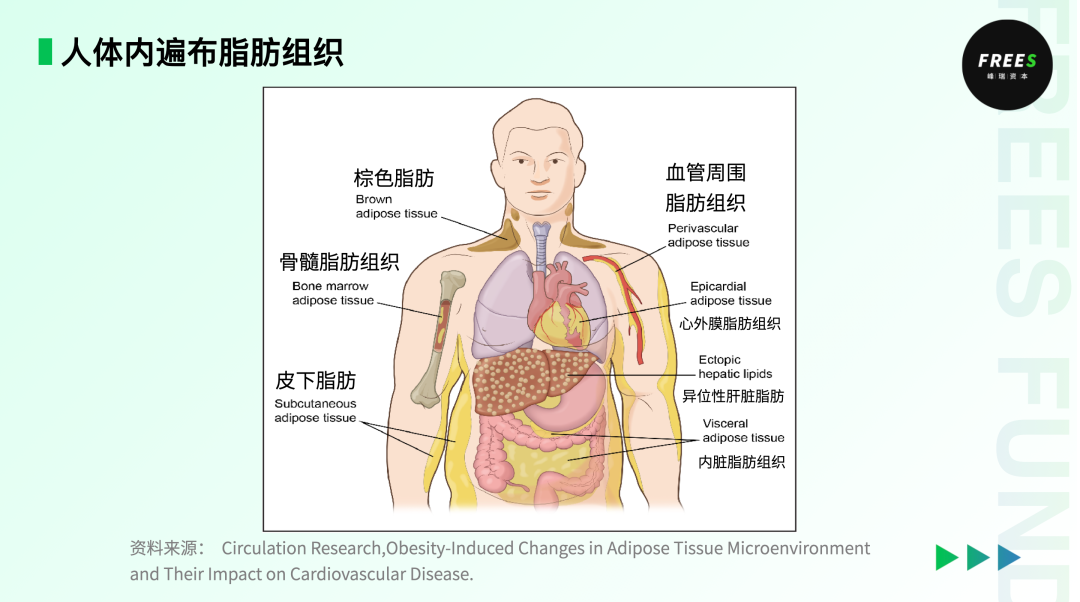
Fat cells fall into three broad categories: brown fat, white fat, and beige fat. Brown and beige fat are mainly distributed on both sides of the neck, or at the shoulders and upper arms. When we feel cold, these fats generate heat to keep us warm. White fat is mainly found in the chest, around internal organs, and under the skin; its primary role is energy storage. Humans have relatively few fat cells in early childhood, after which they multiply rapidly, stabilizing at around 30 billion after puberty. Each fat cell contains triglycerides — the core of obesity. After adulthood, the number of fat cells remains essentially stable, but their volume can vary enormously; a single fat cell can expand up to 1,000 times. In this sense, there may be no upper limit to obesity. We care so much about obesity because it is not only a disease in itself but also raises the risk of cardiovascular and cerebrovascular diseases, high blood sugar, and other conditions.
/ 02 / How Does Obesity Occur?
▎A Physiological Perspective: Unpacking the Pathological Mechanisms
A paper published in Biomolecules, "Obesity–An Update on the Basic Pathophysiology and Review of Recent Therapeutic Advances," summarizes the scientific findings on obesity mechanisms to date. The authors note: "The pathophysiological mechanisms of these metabolic diseases are at the crossroads of different highly specialized medical fields, such as genetics, cellular and molecular biology, endocrinology, etc. (We) can now only reveal (the underlying mechanisms) through 'omics' technologies, which may be the closest to precision medicine approaches."
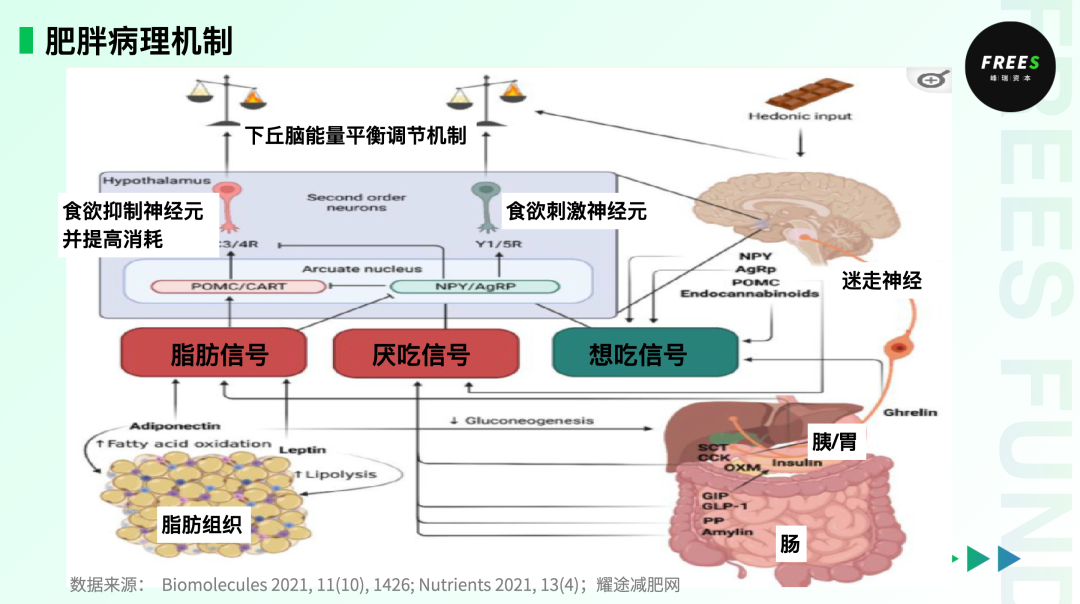
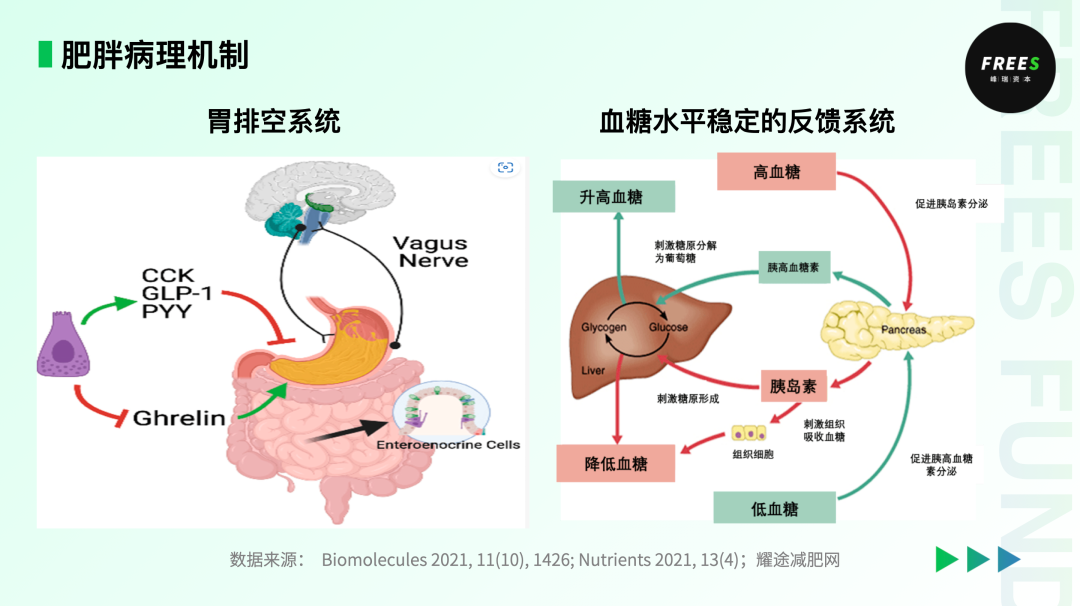
The body's energy balance is influenced and controlled by multiple organs and systems, including the central nervous system, adipose tissue, and the gut, liver, and pancreas. The brain's appetite control center is located primarily in the arcuate nucleus (ARC) of the hypothalamus, which contains two types of neurons that regulate appetite: AgRP neurons stimulate appetite, while POMC neurons suppress it. Ghrelin, secreted by the gastrointestinal tract, acts on specific hypothalamic neurons to generate hunger; leptin, secreted by adipose tissue, acts on different hypothalamic neurons to suppress appetite. Leptin and ghrelin are perpetually locked in attack and defense.
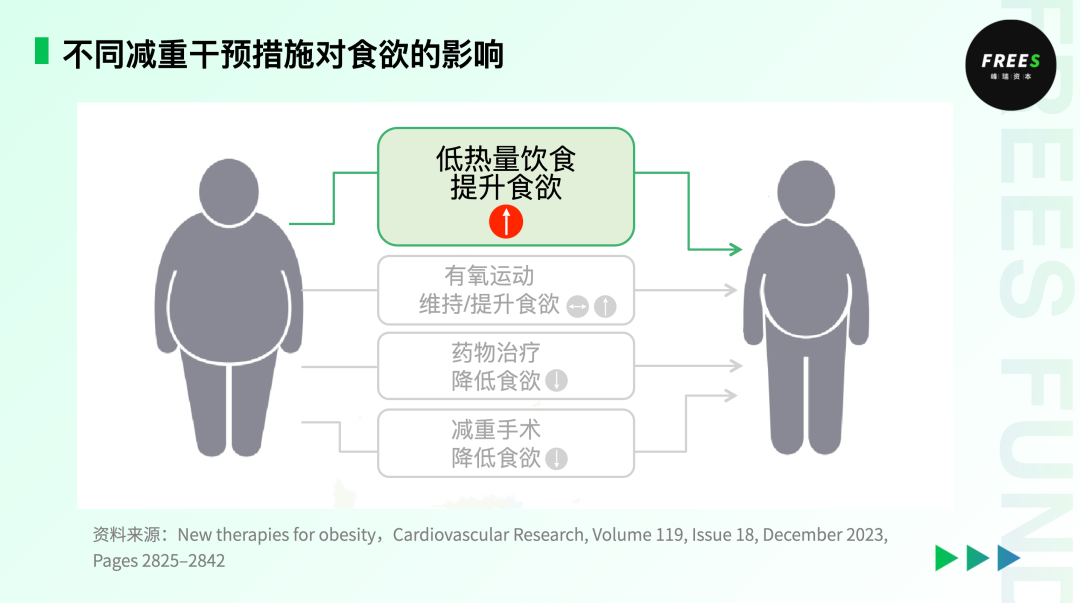
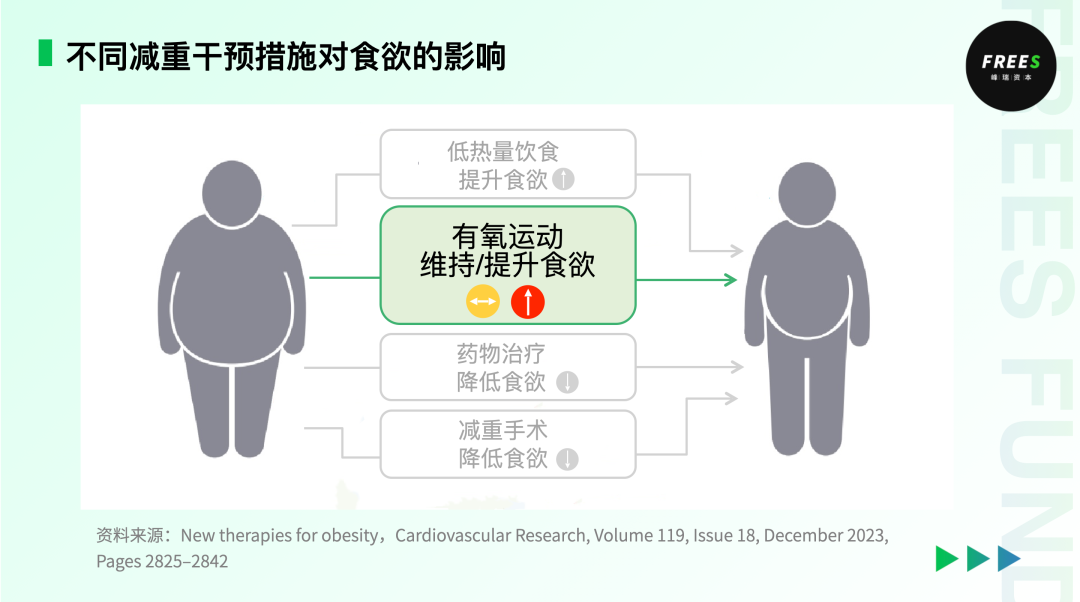
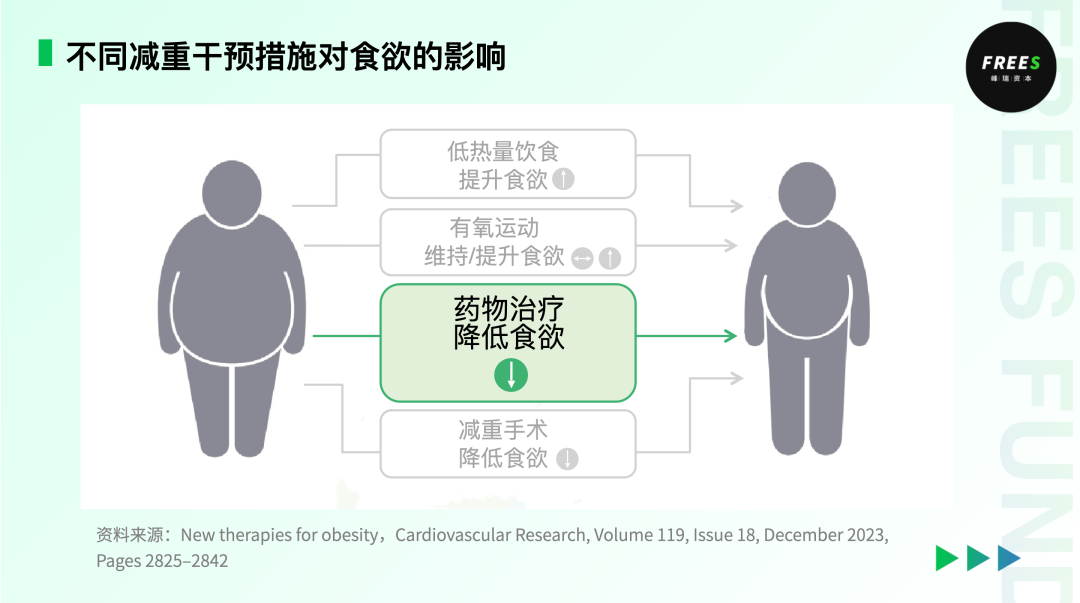
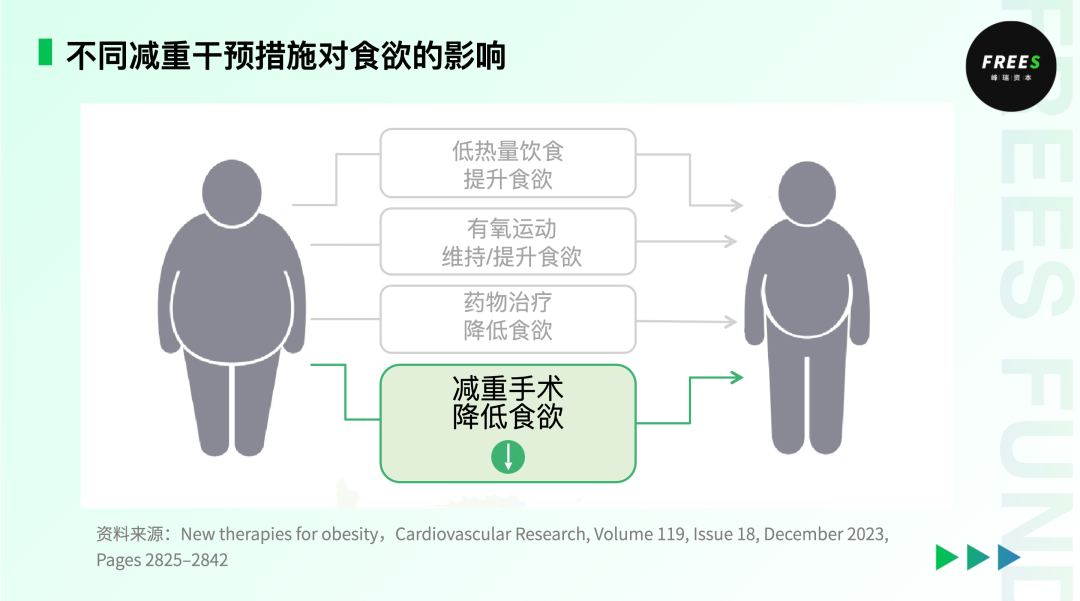
So which of our everyday weight-loss measures actually suppress appetite? A paper published in Cardiovascular Research, "New therapies for obesity," examined how four different weight-loss approaches affect appetite: low-calorie diets, aerobic exercise, drug therapy, and bariatric surgery:
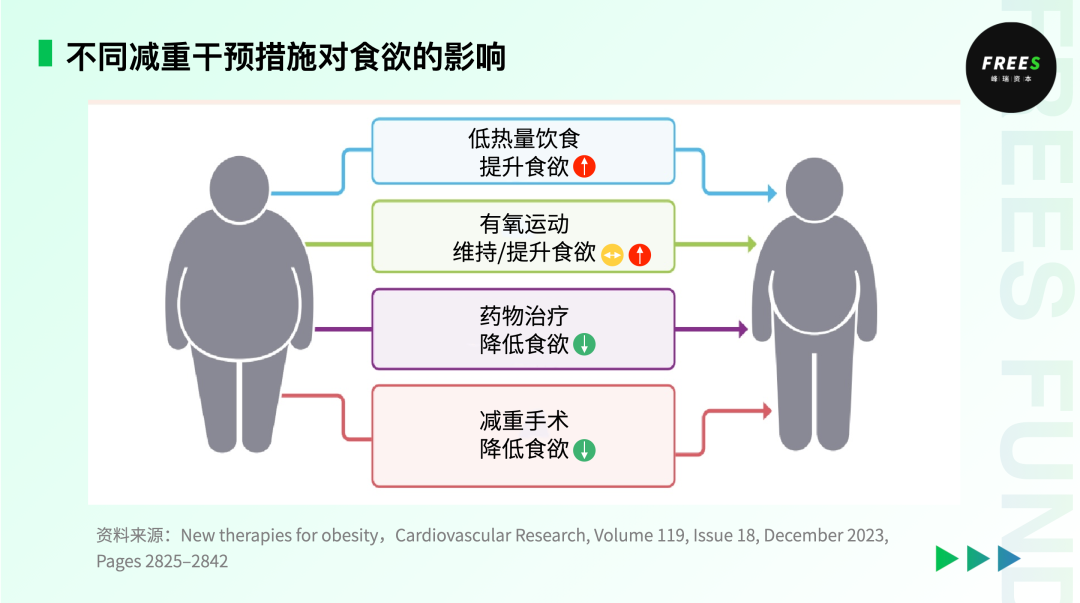
- Low-calorie diets increase appetite. They typically create an energy deficit, triggering stronger hunger and thus boosting appetite.
- Aerobic exercise maintains or increases appetite. While obese patients experience temporary subjective appetite suppression during exercise, energy intake is minimally affected. Specifically with aerobic exercise, hunger slightly increases in a fasted state, followed by increased post-meal satiety, but without significant change in overall energy intake.
- Drug therapy reduces appetite. Anti-obesity medications work mainly through two mechanisms: dampening "wanting" signals to counteract the desire to eat, or amplifying "liking" signals to improve impaired satiety.
- Bariatric surgery reduces appetite. Gastric resection or intestinal bypass surgery lowers ghrelin levels, reducing appetite and consequently food intake.
The author of New Therapies for Obesity argues that obesity might be understood as a disorder of appetite regulation, with increased hunger or decreased satiety as its primary symptoms. Lifestyle interventions alone cannot effectively reduce hunger or increase satiety. Whether through low-calorie diets or exercise, the ultimate effect is to stimulate appetite. The feedback loop controlling long-term energy intake may be more powerful than the one controlling energy expenditure. When we shift perspective back to the individual, absorption and metabolic rates vary from person to person, and suitable weight-loss methods differ accordingly. Below, we'll examine in detail the advantages and disadvantages of different approaches — low-calorie diets, aerobic exercise, drug therapy, and bariatric surgery — and which populations they suit.
From an Evolutionary Perspective, Obesity Is a Mismatch Disease
In The Story of the Human Body, Daniel Lieberman, professor of human evolutionary biology at Harvard University, examines human health and disease through an evolutionary lens and introduces the concept of "mismatch diseases."
In his view, many human traits evolved to suit the environments our ancestors experienced, not the modern environments we've created through culture. Obesity, diabetes, and an increasing number of mismatch diseases are the result of our bodies poorly or insufficiently adapting to these new environments.
Looking back at human history, the hunter-gatherer era lasted roughly 200,000 years, the agricultural era nearly 10,000 years, and the industrial era only about 200 years. Many of our anatomical and physiological features remain adaptations to the hunter-gatherer environment.
In that era, our ancestors survived on foraged fruits and hunted game, frequently facing cyclical food shortages. Only those genes that allowed rapid, efficient extraction and storage of nutrients from limited food could be passed on. This led humans to evolve a preference for energy-dense foods and the ability to store fat efficiently. Avoiding unnecessary energy expenditure also became an instinct.
Yet in just the past few centuries — especially the past few decades — human labor and lifestyles have transformed dramatically. The pressure to find food and ensure survival has plummeted, while human anatomy and physiology haven't had sufficient time to evolve to match this rapid change.
Today, we no longer need to traverse mountains for food, or even "hoe at noon in the heat." Lying at home, we order delivery, and food arrives in our hands. Meanwhile, food supply has increased substantially, with higher caloric content, more processing, and easier digestion and absorption. But our energy expenditure has declined steadily due to technological convenience, creating a severe caloric imbalance. As Lieberman puts it, humanity is steadily sinking into the mire of increasingly frequent mismatch diseases.
How Should We Address Obesity?
As mentioned above, current mainstream weight-control strategies fall into four categories: low-calorie diets, aerobic exercise, drug therapy, and bariatric surgery. Let's examine each approach's characteristics and potential pitfalls in detail.
Diet: The Fat vs. Sugar Controversy
A counterintuitive truth: low-fat diets alone don't control weight as effectively as people imagine, and blindly avoiding beneficial and necessary fats can actually backfire. Americans have already taken this wrong turn for us.
In 1955, U.S. President Dwight D. Eisenhower suffered a heart attack. Following his first heart attack, his medical team prescribed lifestyle changes, with a key recommendation being a low-fat, low-cholesterol, high-carbohydrate diet.
At the time, heart disease was already epidemic in America. Two schools of thought proposed competing hypotheses for its cause. Led by British physiologist John Yudkin, one camp argued sugar was the primary culprit. Ancel Keys, a professor at the University of Minnesota, believed fat was to blame.
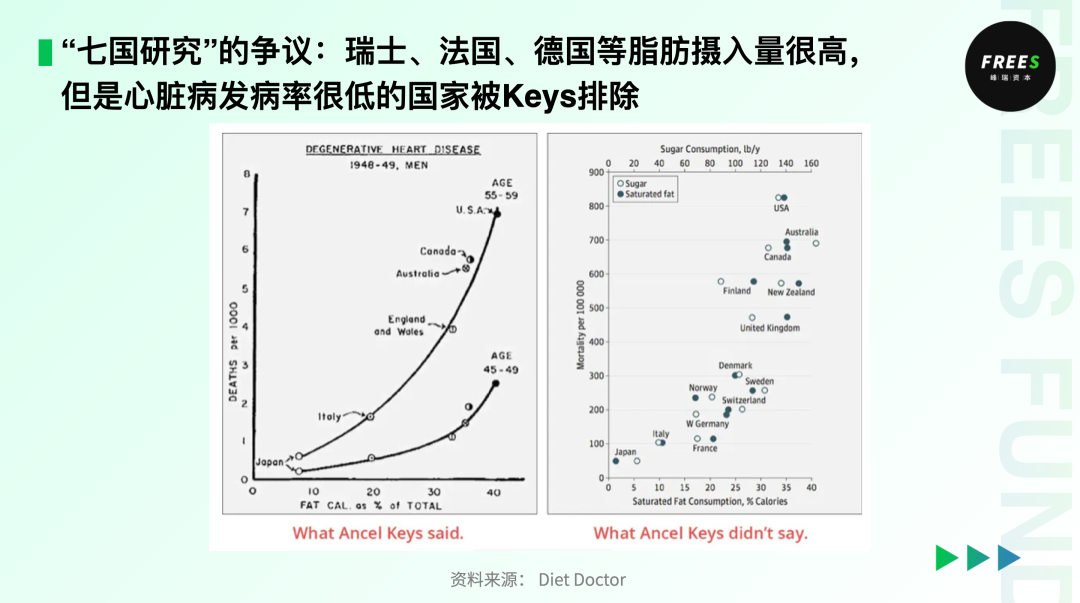
Keys claimed that starting in 1958, he conducted a survey covering seven countries — Italy, Greece, Yugoslavia, Finland, the Netherlands, Japan, and the United States — the famous "Seven Countries Study." The results showed that across these nations, heart disease deaths increased alongside fat consumption.
Keys's conclusions were subsequently adopted by U.S. public health authorities. In 1980, the U.S. government issued its first Dietary Guidelines for Americans, recommending that Americans follow a low-fat diet with daily fat intake not exceeding 30% of total energy. Unexpectedly, over the following two decades, American obesity and heart disease rates surged dramatically. Meanwhile, Eisenhower — who had strictly followed the "low-fat" advice — had his gallbladder removed, developed diabetes and stroke, and ultimately died of heart failure within 14 years of his first attack.
These anomalies drew increasing attention from researchers. According to scholars including Katherine Pett, someone reanalyzed the Seven Countries Study data in 1999 and found that sugar correlated more strongly with heart disease than saturated fat did, proving sugar — not saturated fat — was the real culprit. Critics also noted that Keys had originally collected data from 22 countries; the seven countries presented were deliberately selected, while data that failed to support his hypothesis was concealed.
In 2010, the American Society for Nutrition stated there was no clear evidence linking dietary fat intake to coronary heart disease or cardiovascular disease. The 2016 edition of the Dietary Guidelines for Americans eliminated limits on cholesterol and fat's percentage of energy intake.
The dangers of excessive sugar consumption for weight gain became increasingly recognized. According to The Lancet's 2016 Global Burden of Disease Risk Factors study, considering exposure levels and severity of disease burden impact, sugar-sweetened beverages' summary exposure value rose 40% between 1990 and 2016. Risks from sugar-sweetened beverages to the cardiovascular and metabolic systems include obesity, type 2 diabetes, hypertension, and cardiometabolic disease-related mortality.
Per WHO recommendations, added sugar intake should ideally be kept below 10% of total daily energy intake — approximately 50 grams, preferably 25 grams. For children, this should be even lower: children aged 4–5 should ideally consume under 16 grams.
The fat-versus-sugar controversy has made people more aware of diet's importance for health. But if the goal is weight loss, what's the sensible path?
First, control energy intake.
The Chinese Expert Consensus on Medical Nutrition Therapy for Overweight/Obesity (2016 Edition) mentions a calorie-restricted balanced diet approach: reducing daily intake by approximately 500 kcal from current consumption. To compensate for this deficit, the body will burn stored carbohydrates and fats.
Second, adjust dietary structure.
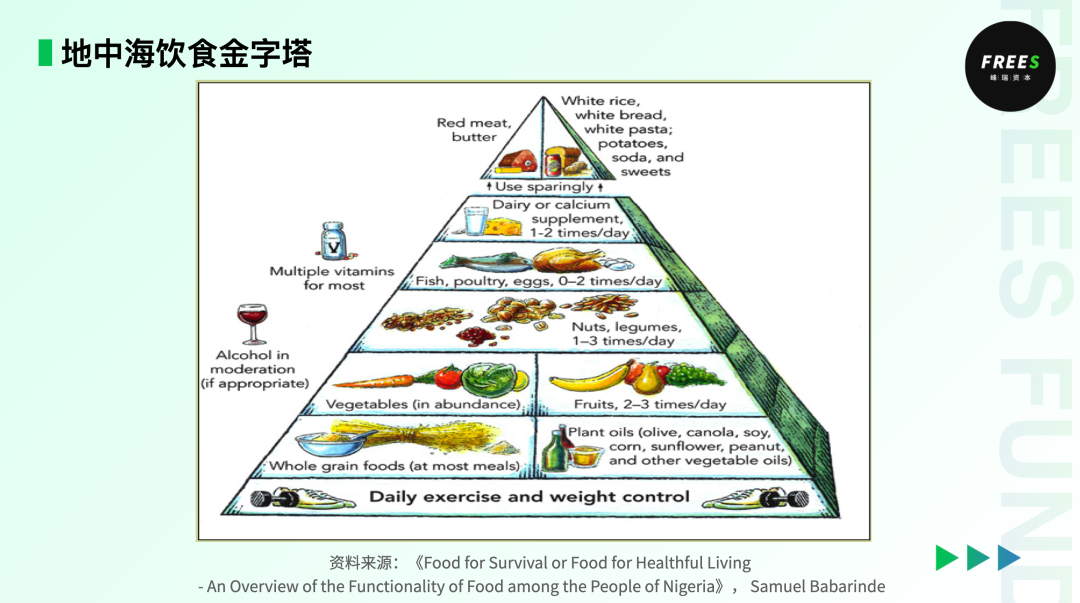
One widely recognized dietary pattern is the "Mediterranean diet." In our previous report FreeS Report 25: Food Investment from the Perspective of China's Dietary Structure, we noted that the "Mediterranean Diet Pyramid" was jointly proposed by Oldways, the Harvard School of Public Health, and the WHO in 1993, primarily based on 1960s dietary patterns in Greece and southern Italy. This dietary pattern is believed to reduce incidence of heart disease, depression, and dementia.
Specifically, Mediterranean dietary habits include:
- Daily consumption of whole grains, fruits, vegetables, olive oil, and nuts
- Fish and seafood at least twice weekly
- Moderate amounts of dairy, eggs, and poultry
- Limited red meat and sweets
- Water as primary beverage, moderate wine consumption
- Cooking methods: primarily low-temperature, slow cooking
- Daily lifestyle: eating with family and friends, afternoon rest, regular exercise

Summary
The effects of fat and sugar on the body aren't absolute; the key lies in controlling quantity. Many obese individuals do need dietary restructuring — both controlling energy intake and adjusting dietary composition.
Exercise: Understanding the Significance of Movement from Underlying Physiological Mechanisms
Having discussed diet, let's turn to exercise. Following the same "adaptation" principle that applies to dietary adjustment, exercise may feel "against human nature," but we can understand it as a medical intervention — humans must increase energy expenditure through exercise to return to equilibrium.
At its core, we can improve athletic performance by understanding biomechanical and exercise physiological systems.
First, the biomechanical system. The human body has three energy systems: the phosphagen (ATP-CP) system, the glycolytic system, and the oxidative system.
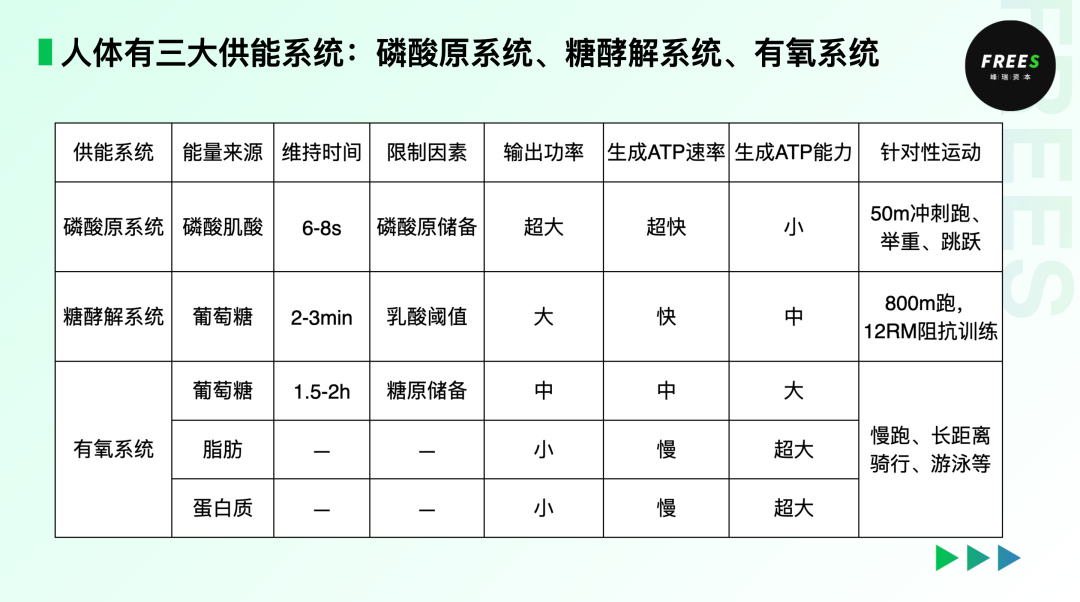
The phosphagen (ATP-CP) system delivers high-intensity energy for short bursts without requiring oxygen. When we sprint, long jump, throw shot put, or lift weights — any activity demanding explosive power — this system fuels our muscles. But that burst typically lasts no more than ten seconds.
The glycolytic system generates energy by breaking down carbohydrates (glycogen and blood glucose), still without oxygen involvement. Though slower to respond than the phosphagen system, it can sustain output for two to three minutes. An 800-meter run draws primarily from this system.
The oxidative system uses carbohydrates, fats, and small amounts of protein to produce energy. It's the main source during rest and low-intensity activities — jogging, long-distance cycling, swimming. Its metabolic pathway is longer, but it yields more energy, which is why lower-intensity exercise actually burns more fat.
From an exercise physiology standpoint, different activities tap different energy sources. In daily life, whether we're still or moving, all three systems contribute simultaneously. But their relative contributions depend mainly on exercise intensity and duration.
Exercise shouldn't be a blind trend-following exercise. Choosing what suits your body is how you actually solve problems or reach goals. If fat loss is your priority, prioritize aerobic training with anaerobic work as supplement. If body recomposition is the goal, flip that ratio.
Still, exercise's impact on weight control pales next to dietary changes. As the saying goes: "Seventy percent diet, thirty percent training." The energy in a 600ml bottle of soda would take an adult 8,500 steps of brisk walking to burn off. Understanding how hard energy is to expend might instill some reverence for both eating and exercise.
Data from New Therapies for Obesity shows that restricting 500 calories daily plus 150 minutes of weekly exercise yields 2% to 5% weight loss over a year. Add full meal-controlled energy restriction plus structured training, and you might hit 10% in a year. Of course, that's a victory reserved for the few.
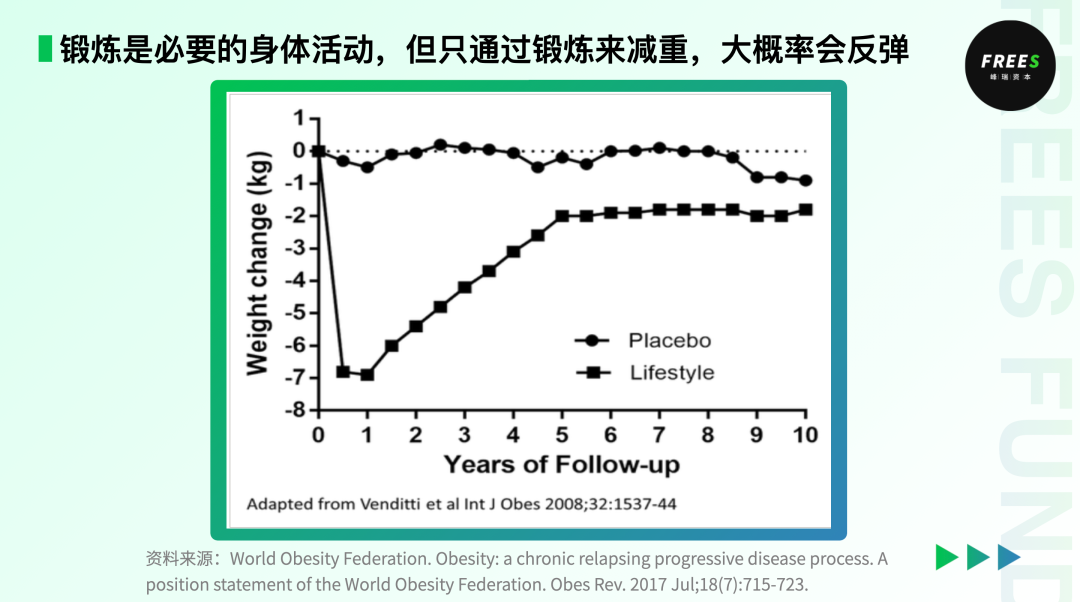
In reality, weight regain after lifestyle intervention is the probable outcome. New Therapies for Obesity notes that weight loss plateaus after about a year of sustained exercise alone; over five years, roughly 80% of lost weight typically returns. Only about 10% to 25% of people maintain weight loss greater than 10% long-term.
Why?
First, from an energy metabolism perspective: during exercise, basal metabolic rate drops — and it drops far more than fat mass declines as a percentage of total body weight. Yet basal metabolism is the body's primary form of energy expenditure. This is known as "metabolic adaptation."
A Current Biology article, "Energy Compensation and Adiposity in Humans," notes that exercise reduces basal metabolic levels, thereby diminishing exercise's fat-burning effects. This phenomenon is most pronounced in people with obesity and older adults, with the greatest impact on those with obesity. Which is why we so often hear the complaint "I exercise and still gain weight." Frustrating, but true: obesity level determines the individual variation in compensation mechanisms.
Metabolic adaptation brings another consequence: even if a dieter's weight rebounds, basal metabolic rate remains suppressed for an extended period, making subsequent weight loss even harder.
"There are two possible causes for this compensatory effect," the authors of "Energy Compensation and Adiposity in Humans" suggest. "One is that exercise increases appetite, leading to greater food intake. The other is that exercise reduces energy expenditure in other areas, such as resting metabolism, to lower the energy cost of exercise." Hence, weight regain becomes highly likely over time.
So from a physiological mechanism perspective, lifestyle intervention alone produces relatively limited medium- to long-term results for most people.
Does that mean we should just lie flat? Of course not!
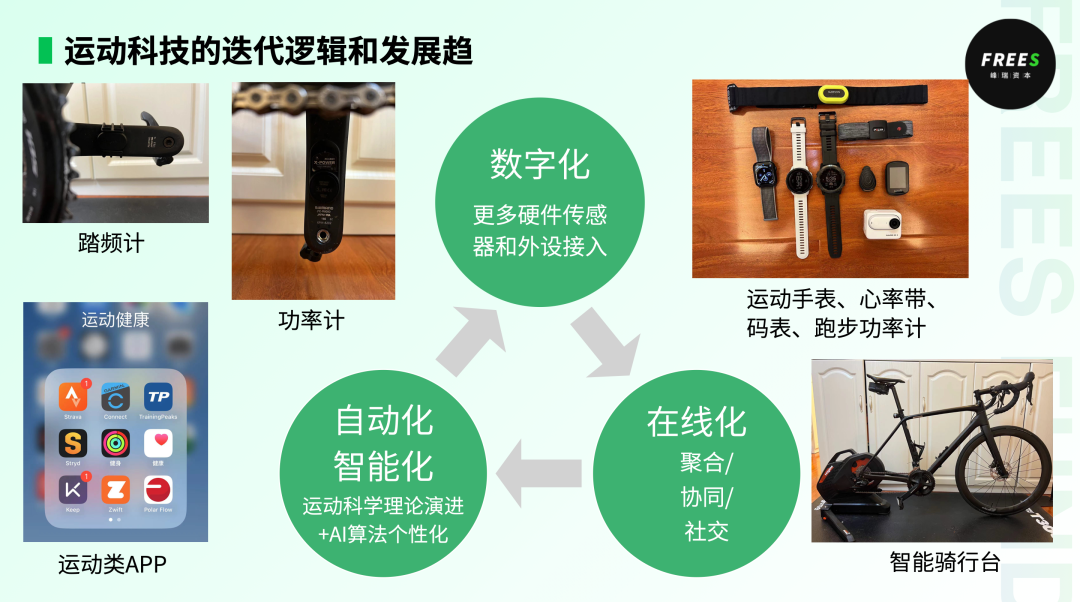
With adjusted expectations, we still need to develop targeted, personalized exercise plans. Or better yet, choose a "competitive" sport you're relatively good at — team sports like soccer, basketball, or baseball; or endurance activities where you compete against yourself like long-distance running, swimming, or yoga — and let dopamine help you beat laziness. Plus, we can leverage various tech-enabled devices to enhance training effectiveness.
While exercise alone may not produce dramatic weight loss long-term, health isn't defined by low body weight. Sensible eating and consistent training will make you happier and stronger.
Key Takeaways
Whether through dietary adjustment or fitness training, single-strategy lifestyle-change weight loss plans mostly control weight only in the short term; long-term rebound is highly probable. But lifestyle adjustments remain beneficial over time — they make people physically and mentally healthier.
Drugs: Miracles Don't Play Out for Everyone
We mentioned earlier that obesity can be viewed as a disorder of appetite regulation, and medication can help control appetite. For a long time, drug therapy didn't receive much recognition from serious medicine due to efficacy or side effect concerns. As understanding of peripheral and central signals and mechanisms involved in weight management and maintenance has deepened, developing more effective and safer weight-loss drugs has become possible.
In the pharmaceutical weight-loss space, semaglutide is currently the hottest name. The original semaglutide product was developed by Danish biopharma Novo Nordisk. It's a human glucagon-like peptide-1 (GLP-1) analog used for diabetes and obesity care.
GLP-1 is an intestinal hormone secreted by the gut that increases satiety, affecting the body through multiple pathways: appetite suppression, delayed gastric emptying, blood glucose regulation. Physiological GLP-1 secretion peaks after meals, signaling fullness to the brain. GLP-1 drugs were originally developed to stimulate insulin secretion for diabetes treatment, then applied to obesity with marked efficacy.
Though it sounds miraculous, that miracle doesn't manifest for everyone.
A study published in Obesity roughly categorized people with obesity into four subtypes: brain-driven hunger obesity, emotional hunger obesity, gut-driven hunger obesity, and slow-burn obesity.

Experimental results suggest that GLP-1 drugs like semaglutide may achieve better weight loss outcomes in people with gut-driven hunger obesity. In other words, before using such medications, it's worth determining whether you fall into this category. A typical manifestation: you feel full after a normal-sized meal, but hunger returns quickly. If not, your obesity may instead be:
- Brain-driven hunger: requiring more food to achieve satiety
- Emotional hunger: using food to relieve anxiety and depression
- Slow-burn: relatively slower metabolism
For these three groups, weight loss through GLP-1 drugs may prove disappointing.
It's also worth noting a clear drawback of such medications: weight rebound upon discontinuation, with speed varying by individual. A study in eClinicalMedicine, a Lancet journal, examining GLP-1 drug efficacy notes that despite their obvious weight-loss effects, maintaining weight becomes extremely difficult once stopped. Within a year of discontinuation, participants typically regain over two-thirds of previously lost weight. The good news: those who exercised during GLP-1 treatment showed no significant tendency toward weight rebound after stopping the drug.
So even with pharmaceutical weight loss, lifestyle changes remain necessary to maintain results or ensure more gradual rebound.
Of course, an unavoidable issue is potential side effects. News reports have documented negative reactions in some "weight-loss shot" recipients, including dizziness, elevated heart rate, fatigue, mild hypoglycemia, and facial skin sagging.
Key Takeaways
"Miracle weight-loss drugs" mainly work by suppressing appetite and regulating gastric emptying, but they're not universally suitable, and effectiveness varies depending on the cause of obesity. After discontinuation, gradual weight rebound is likely; supplementing with dietary and exercise adjustments may prolong the drug's weight-loss effects.
Bariatric Surgery: Dramatic Results, Significant Drawbacks
Bariatric surgery directly reduces appetite. Compared with diet adjustment, exercise, and medication, surgical weight loss is relatively straightforward.
Bariatric surgery mainly follows two approaches. The first is gastric resection, which removes about 80% of the stomach to reduce its volume and restrict food intake. Since the removed tissue includes the gastric fundus — where ghrelin is produced — ghrelin levels drop, suppressing appetite. The second is gastrointestinal bypass, which reroutes the path food takes through the digestive tract. After surgery, food enters only the upper portion of the stomach, bypassing the lower stomach and part of the small intestine. This reduces nutrient absorption, lowers ghrelin levels, and stimulates GLP-1 secretion in the intestines.
However, despite the notable effectiveness of both procedures, the bariatric surgery industry remains constrained. Currently, these operations are only suitable for certain severely obese populations.
For one, existing medical resources cannot fully meet market demand. For another, surgery is inherently invasive, carrying risks of intraoperative and postoperative complications — relatively few people are willing to undergo such drastic measures for weight loss. Additionally, surgery may bring long-term effects. Since it alters the pathways for digestion and absorption, patients may need lifelong supplementation with relatively high doses of multivitamins and trace elements.
Summary
For severely obese patients, surgery offers relatively direct and durable results, but most people don't need to go under the knife.
Market Opportunities Related to Weight Control
As China's weight loss and weight management market grows year by year, numerous potential opportunities have emerged. In this report, we focus on analyzing innovation opportunities in two niche areas: sugar substitutes and weight-loss drugs.
Sweeteners and DGI Foods
As we mentioned earlier, excessive sugar intake is an important cause of weight gain. When people consume more sugar than needed for physiological functions, the surplus is stored as fat in the body.
In the early days, using sugar substitutes to reduce intake of sucrose, maltose, fructose, and other conventional sugars was a relatively low-cost weight-loss option.
What journey has our sugar consumption been through?
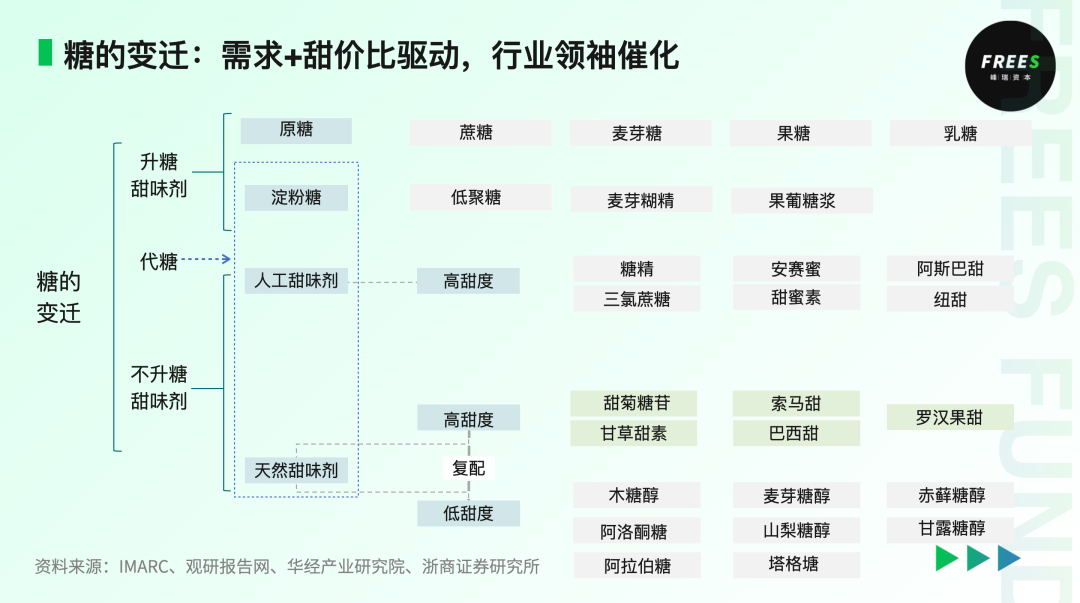
The first generation of sweeteners was represented by sucrose. Derived mainly from sugar beets and sugarcane, sucrose has thousands of years of history.
The second generation was primarily high-fructose corn syrup (HFCS), which offers higher sweetness per unit cost than sucrose. Early on, leading beverages including Coca-Cola and Pepsi mostly used HFCS. In 1984, HFCS surpassed sucrose for the first time to become the dominant second-generation sweetener.
However, excessive fructose intake increases the burden on the liver; the portion that cannot be metabolized is converted to visceral fat. So if your physical examination indicates fatty liver, you should pay attention to whether your daily fructose intake is excessive.
The third generation consists mainly of artificially synthesized high-intensity sweeteners. These dramatically reduce calorie content while maintaining high sweetness-to-cost ratios, but researchers have never stopped questioning their safety. Most sugar-free beverages on the market today use artificially synthesized high-intensity sweeteners — such as aspartame and sucralose, which we all know — supplemented with small amounts of natural low-intensity sweeteners.
The fourth generation is natural sweeteners. These are mainly extracted from nature or produced through microbial fermentation, making them healthier than artificial alternatives. As synthetic biology continues to achieve breakthrough applications in the sugar substitute field, more and more natural high-intensity sweeteners are appearing in the market. Consequently, natural sweeteners are steadily capturing market share from artificial ones.
Natural high-intensity sweeteners have three typical representatives: brazzein, thaumatin, and stevia.
- Brazzein: Extremely high sweetness, thousands of times that of sucrose. After entering the human body, it is converted to amino acids and then absorbed and metabolized, causing no glycemic response and avoiding the bitter aftertaste associated with some previous artificial sweeteners.
- Thaumatin: Refreshing sweetness, no off-tastes, and long-lasting. Additionally, thaumatin has excellent processing stability — it remains stable during pasteurization and baking, and common preservatives do not affect it.
- Stevia: High sweetness, low calories, stable physical properties, and relatively good sweetness-to-cost ratio, with slight bitter and licorice notes. Its sweetness is 200–450 times that of sucrose, while its caloric content is only 1/300 of sucrose's.
Waterdrop, a portfolio company of FreeS Fund, is a synthetic biology company dedicated to producing high-value proteins. Their main products include brazzein and thaumatin.
In actual production, sweeteners are more often used in combination to increase sweetness and reduce costs; minimize undesirable tastes and enhance flavor; and improve and ensure product stability. A promising future direction is combining high-intensity natural sweeteners with low-intensity natural sweeteners to achieve evolution toward both health benefits and desirable taste.
The Healthy China Initiative (2019–2030) proposes advocating that food producers and operators use natural sweetening substances and sweeteners permitted by food safety standards to replace sucrose. It encourages urban populations with high sugar intake to reduce consumption of sucrose-containing beverages and sweets, choosing instead beverages and foods produced with natural sweetening substances and sweeteners as sucrose replacements.
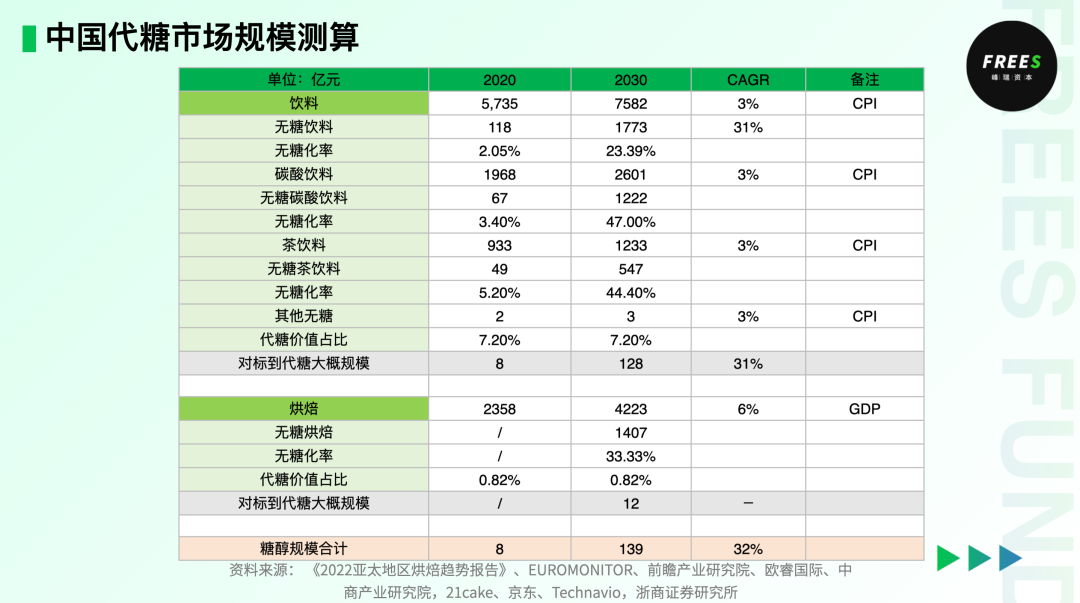
Driven by the demand for "both good taste and health," China's sugar-free market is accelerating its expansion. According to estimates by Zheshang Securities Research Institute, if China's sugar substitute market (covering only beverages and baking) reaches levels comparable to developed countries, it could approach nearly 14 billion RMB by 2030, with a compound annual growth rate of about 30% over ten years.
Beyond controlling sugar intake, we need to pay attention to another concept — the Glycemic Index (GI). GI indicates how quickly and how much blood sugar rises after consuming carbohydrate-containing foods. Generally, a higher GI value means greater blood sugar fluctuation and faster rise; a lower GI value indicates smaller fluctuation and slower rise.
- Low-GI foods: GI below 55, e.g., multigrain bread, apples, oats.
- Medium-GI foods: GI between 55 and 70, e.g., rice noodles, sweet potatoes, brown rice.
- High-GI foods: GI above 70, e.g., noodles, steamed buns, pumpkin.
Choosing low-GI foods can bring many health benefits, such as slowing blood sugar rise, reducing fat accumulation, and prolonging satiety.
In the energy-control food sector, Methuselah, another FreeS Fund portfolio company, has developed a rare complete medical nutrition food business line encompassing foods for special medical purposes (FSMP), low-GI products, and energy-controlled weight management products. It has entered over 700 top-tier tertiary hospitals and served more than 10 million patients, while also bringing health foods for scientific sugar and energy control under medical nutrition guidance to more consumers — a representative brand amid the new round of professional and technological upgrading in the food industry.
For more on innovation opportunities in the food sector, we have provided detailed analysis in What Humans Will Eat in the Future | FreeS Report 27. Welcome to click the link and read.
Weight-Loss Drugs: Beyond Efficacy, Safety and Compliance Are Future R&D Priorities
According to Pfizer's report projections, the U.S. market for GLP-1 drugs in type 2 diabetes and obesity could reach $90 billion by 2030, potentially displacing PD-1/L1 drugs as the "world's top-selling drug class." The type 2 diabetes drug market would account for approximately $35–40 billion, and the weight-loss drug market about $50–55 billion.

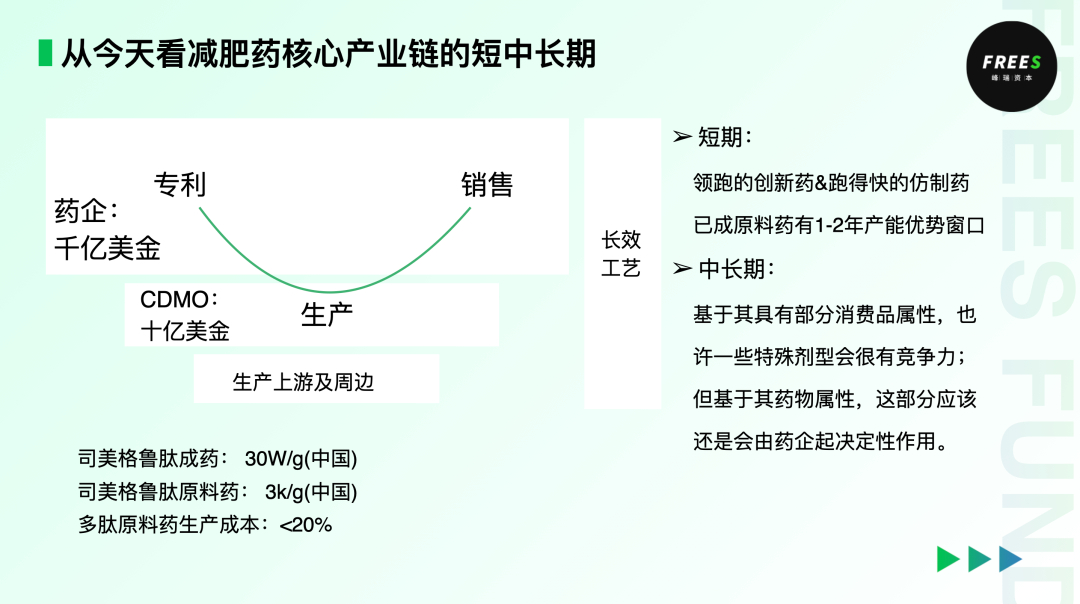
Because weight-loss drugs possess certain consumer product attributes, special formulations meeting specific population needs can stand out from competition. Yet their pharmaceutical nature seems to dictate that this hundred-billion-dollar market may be "carved up" by the serious medical industry.
The core industry chain for weight-loss drugs follows a "smile curve." Currently, most profits remain concentrated in leading pharmaceutical companies that hold patents and control sales channels. In the short term, companies with first-mover advantages and API (active pharmaceutical ingredient) enterprises will enjoy a certain window period. But in the medium to long term, as over 100 related pipelines advance globally, competition in the weight-loss drug market will intensify rapidly.
As a representative of GLP-1 drugs, Novo Nordisk's semaglutide has achieved commercial success. Novo Nordisk's 2023 financial report shows that Wegovy (the brand name for its semaglutide product) saw sales surge 406% to $4.6 billion, leading the global GLP-1 segment by a wide margin.
Eli Lilly and Company, which alongside Novo Nordisk is known as one of the "GLP-1 dual giants," developed another GLP-1 drug, tirzepatide. On November 8, 2023, after tirzepatide was approved for weight loss, it generated $176 million in revenue for Eli Lilly in less than two months.
Multinational pharmaceutical giant Roche is also increasing its bet on the weight-loss drug track. At the end of 2023, Roche announced the $3.1 billion acquisition of Carmot Therapeutics, an obesity treatment drug manufacturer. Through this, Roche will gain a series of GLP-1 (glucagon-like peptide-1) agonist-based anti-obesity and diabetes drugs.
Interestingly, five years before this deal, Eli Lilly had obtained Roche's GLP-1 program from Chugai (Roche's Japanese subsidiary) for a $50 million upfront payment. In just five years, Roche paid a 60x premium to bring GLP-1 drugs back under its umbrella — a vivid illustration of how hot the novel weight-loss drug market has become.
Currently, as the most highly regarded weight-loss drug category, with efficacy — the core issue — largely resolved, safety and compliance have become the main considerations for GLP-1 drug development. Medication compliance means patients can take drugs according to the prescribed dosage, frequency, and timing.
Future R&D directions for weight-loss drugs mainly fall into three areas:
First, extending the duration of drug effects. For instance, reducing dosing frequency from once weekly to once monthly — lower frequency typically improves compliance.
Second, making administration more convenient. Beyond injectables, developing oral formulations could serve a far broader population of overweight individuals. Oral drugs also tend to support better medication compliance than injections. This may partly explain why small-molecule weight-loss drugs have become such a hot R&D area.
Third, continuously refining functionality. GLP-1 drugs used alone for weight loss can lead to muscle loss in some patients. Several pharmaceutical companies are now exploring combinations of GLP-1 with other agents, enabling consumers to lose weight while gaining or preserving muscle.
Preemptive Care: "The Highest Physician Treats What Is Not Yet Ill"
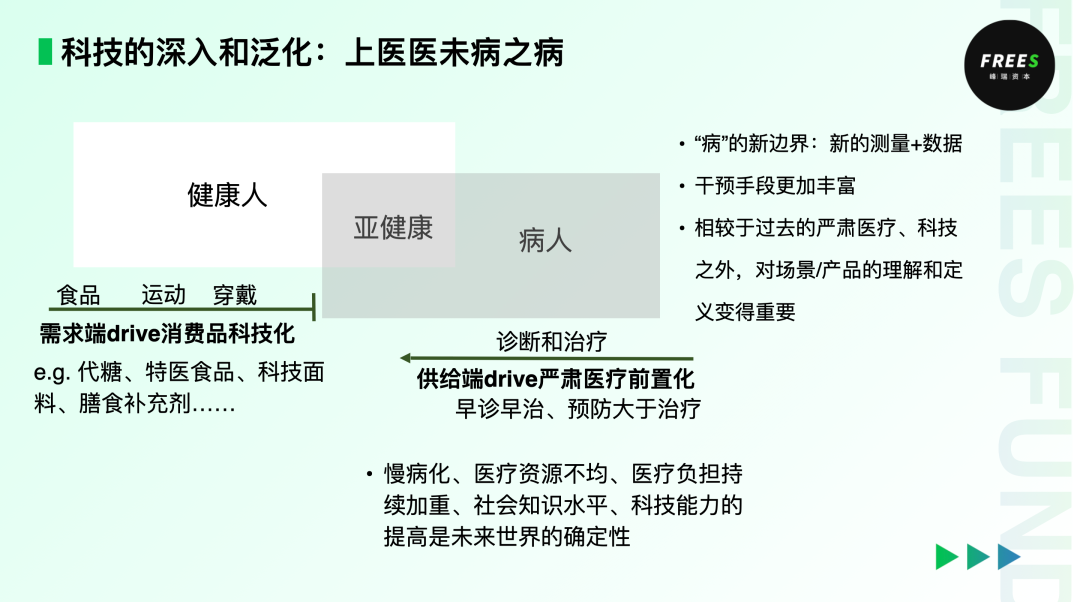
The legendary physician Sun Simiao wrote in Essential Formulas for Emergencies Worth a Thousand Gold: "Eliminate troubles before they arise, treat diseases before they manifest, and practice medicine before crisis occurs." From ancient times to the present, "the highest physician treats what is not yet ill" has described the pinnacle of medical excellence. As technology penetrates and generalizes across medicine, the goal of earlier diagnosis and intervention — preventing disease before it arrives, eliminating it before it emerges, curing it before it worsens — is gradually shifting from distant aspiration to achievable reality.
Just as exercise and dietary adjustments can intervene before weight issues become clinical disease. When intervention tools extend beyond serious medical care into consumer products, startups in this space might reconsider their approach: building on medical or technological foundations, they should devote more attention to product development and concrete application scenarios. For example, improving the taste of sugar substitutes and foods for special medical purposes to help people control energy intake; lowering the barrier to using wearable devices so more physiological indicators can be monitored, giving people more intuitive, precise visibility into how their bodies are changing.
This principle extends far beyond weight management. Applied to the broader biopharmaceutical industry, "treating what is not yet ill" is equally relevant. A person's trajectory from health to sub-health to illness is typically gradual — there is ample room for proactive measures. Most patients with liver cirrhosis or liver cancer seek medical attention only after severe symptoms appear, by which point diagnosis and treatment are often extremely difficult. If highly accessible early screening could identify and confirm conditions at the NASH (non-alcoholic steatohepatitis) stage, or even before substantive liver changes occur, the difficulty of cure could be substantially reduced, effectively easing the medical burden on families and society.
From this, we anticipate several potential trends in healthcare and drug R&D:
First, earlier diagnosis and disease definition will grow increasingly important, likely requiring new computational, measurement, and modulation technologies to digitize physiological indicators for more precise recording and more effective prediction.
Second, against the backdrop of preemptive diagnosis, we can deploy richer intervention tools rather than limiting ourselves to serious medical care alone.
Final Thoughts
Returning to life itself: when it comes to specific methods of weight control, whether you choose lifestyle adjustments, weight-loss drugs, or surgery, results will ultimately vary from person to person. After all, everyone absorbs and metabolizes at different rates — the key is choosing a scientific approach that suits you.
As The Story of the Human Body puts it: "If the rich and complex evolutionary history of our species teaches one useful lesson, it is that culture does not allow us to transcend our biological conditions... This world is not perfect, and neither is our body. But it is the only body we have, and it deserves to be enjoyed, nurtured, and protected."
Every unique one of you deserves a healthier, more vibrant body.
Reader Engagement In the weight loss and weight management market, what innovation opportunities do you see? What weight-loss methods have you tried?
Share your thoughts in the comments. By 17:00 on April 2, 2024, the five most thoughtful commenters will receive a wellness gift package from FreeS Fund, including a copy of The Story of the Human Body and DGI snacks from Masyala.

▲ Li Xiang x Feng Li: Key Dates and Events to Watch in 2024 | Feng Li Column ▲ What Will Humans Eat in the Future? | FreeS Report 27 ▲ Deep Dive: Unpacking the NEV Sales and Aftermarket Services Landscape | FreeS Report 35 ▲ ▲ "The Higher You Stand, the Farther You See": The Origins and Future of the Satellite Communications Space Race | FreeS Report 34 ▲ How Far Are We From "Ready Player One"? The Technical Challenges of XR Through the Lens of Apple Vision Pro | FreeS Report 33 ▲ FreeS Report 25: Food Investment Through the Lens of China's Dietary Structure
Star the FreeS Fund WeChat official account to get timely business insights delivered to your feed.