Based on the underlying principles, preventing and controlling COVID-19.

4. The virus hijacks the cell's nutrients and transcription machinery to make thousands upon thousands of copies of itself.
This article was written by Wang An, founder of Digital Heaven, a portfolio company of Linear Capital. We found it highly educational and recommend it to our readers.
Author's note: All key concepts in this article are linked to Baidu Baike or authoritative academic platforms.
The prerequisite for solving a problem is understanding it.
Too many half-baked answers circulate online. Though well-intentioned, personal anecdotes labeled "worked for me" rarely hold up to scrutiny. Only by returning to first principles can we cut through the noise.
COVID-19 damage to the human body is progressive. Let's trace its steps:
- Virus enters the respiratory mucus layer
- Virus locates ACE2 enzymes on human cell surfaces
- Virus enters the cell
- Virus hijacks cellular nutrients and transcription machinery to replicate tens of thousands of copies
- Viral particles burst through the host cell and begin infecting surrounding cells
- The immune system engages the viral horde in combat
- The immune system, struggling, raises body temperature to boost individual immune cell effectiveness — this is fever
- If the immune system remains overwhelmed, the virus continues down the respiratory tract into the lungs, causing diminished lung function, dropping blood oxygen, and insufficient energy supply to cells throughout the body. Oxygen supplementation becomes necessary
- The episode generally ends with total viral elimination, though outcomes range from mild to severe
Steps 1–4 constitute the incubation period; everything after is the acute phase. As you can see, the virus operates through a lengthy process inside the body. The longer the pipeline, the higher the attrition rate. If we want that attrition, we can set up barriers at every stage. We can roughly model viral damage with this formula:
Viral damage to human body = (Inhaled viral load - Antibody quantity × Antibody efficacy) × Cell entry success rate × Infected cell elimination rate during incubation × 10,000 - Immune cell combat effectiveness - Antiviral drug suppression effect
Next, we'll break down each step and examine how to reduce harm at every point.
1. How to reduce inhaled virus reaching the respiratory tract
Theoretically, the virus can invade beyond the respiratory tract — corneal and anal cells also carry ACE2 receptors. But in the Omicron era, everyday protection need not be so extreme; respiratory defense suffices.
The WHO's standard advice has three points: maintain social distance, wear masks, and wash hands frequently. These three are about distancing from the virus — low cost, effective against early COVID strains. But Omicron's transmissibility is now so high that the virus is everywhere, impossible to avoid. We need supplementary external virucidal measures.
What can kill the virus outside the body? China's National Health Commission's Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 9) is explicit: coronaviruses are sensitive to ultraviolet light and heat. 56°C for 30 minutes, ether, 75% ethanol, chlorine-containing disinfectants, peracetic acid, and chloroform and other lipid solvents can effectively inactivate the virus.
UV light, alcohol, and chlorine-based disinfectants each have suitable scenarios and caveats:
- UV light must not irradiate human bodies or plants
- Alcohol is flammable and unfriendly to pregnant women
- Hypochlorous acid and 84 disinfectant have strong oxidizing properties that can bleach clothing
Practical external virucidal measures:
- Use travel-size spray bottles to disinfect surrounding air frequently (alcohol is flammable; large bottles are hazardous)
- Spray alcohol on clothing upon returning home, or use UV sterilization lamps/cabinets
Beyond external virucidal measures, two expulsion measures are important:
- Nasal rinsing after returning home
- Expectorating and throat clearing
When the virus enters the nasal cavity, it first sticks to nasal hairs or nasal mucus, then randomly seeks out human cell ACE2 receptors. Before the virus enters your nasal cavity and before symptoms erupt, there is a window to physically clear it out.
No need for a neti pot — cotton swabs work. Use saline if you're particular; plain water works too. Dip a swab in saline, insert into the nostril, and clean out mucus, nasal crusts, and some nasal epithelial cells. These epithelial cells may already be infected but still in incubation — clear them out together.
Expectorating and throat clearing work similarly: physically expelling latent virus.
Some suggest gargling with baijiu. This isn't entirely useless. But alcohol doesn't selectively kill COVID-19 — it's also harmful to oral cells. Not suitable as a daily protective measure.
2. How to reduce virus that successfully locates cells
After entering nasal mucus, not all viruses find and bind to human cells. The body's immune cells patrol constantly, eliminating invading pathogens.
Immune cells are tiny — tens of thousands clustered together are merely pinhead-sized. But viruses are smaller still. The size difference is like an elephant patrolling its territory: can it notice an invading ant? Even if noticed, is the ant beneficial or harmful? The elephant cannot instantly judge; without judgment, it won't act.
Viruses are merely organic molecules containing proteins and nucleic acids. Nutrient or pathogen — how to distinguish?
The key is antibodies.
Antibodies are proteins generated by the human immune system. People are easily misled by the name, assuming antibodies kill viruses. They don't. Their purpose is identifying targets for killing.
Different antibodies can chemically react with and bind to different antigens.
What are antigens? Antigens are pathogen characteristics. Below is the molecular structure of SARS-CoV-2:
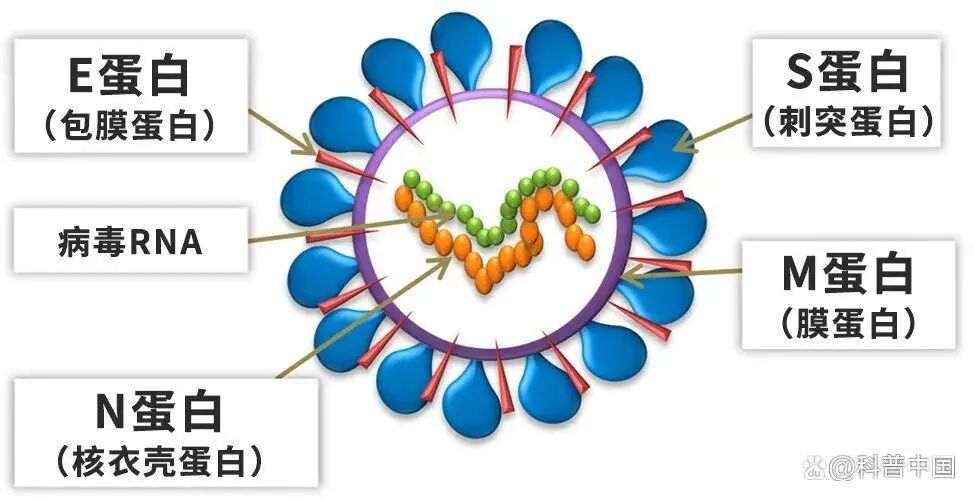
Our antigen tests detect whether viral molecular structures meet specified criteria. Most antigen reagents simultaneously test for the virus's S protein and N protein, reducing false negatives from viral variation.
Of course, those few-yuan reagents have limited sensitivity — they won't detect the virus below a certain concentration.
So when SARS-CoV-2 enters the nasal cavity and encounters antibodies, the antibodies chemically react with viral surface antigens and adhere. Now immune cells recognize: "Oh, a little thing coated in antibodies — you're here to harm me. I'll eliminate you."
The image below is from the documentary Curiosity: Cell Wars.
- The small black spheres are viruses
- The white proteins stuck to the black viral shells are antibodies
- The enormous, flesh-colored, tentacled background entities are immune cells

Here the viruses are not only antibody-coated, but multiple viruses are glued together by antibodies — dramatically improving immune cell elimination efficiency.
Without antibodies in the body, viruses roam unchecked. Some wonder: why this complexity? Why can't immune cells directly kill viruses?
This requires understanding immune system elimination principles. Imagine the body has a hypochlorous acid disinfectant factory. Patrolling immune cells carry this disinfectant, but they cannot spray it everywhere — that would damage the body's own healthy cells. (Cytokine storms and certain autoimmune diseases occur when immune cells attack healthy self-cells.)
So immune cells can only grab pathogens at close range and secrete hypochlorous acid, using this strong oxidizer to destroy them. Essentially, it's a self-triggering chemical reaction.
Antibodies are the chemical intermediary connecting both ends: one side adheres to the pathogen, the other to immune cells.
Without antibodies, viruses bouncing off immune cells simply ricochet away, neither interacting nor engaging.
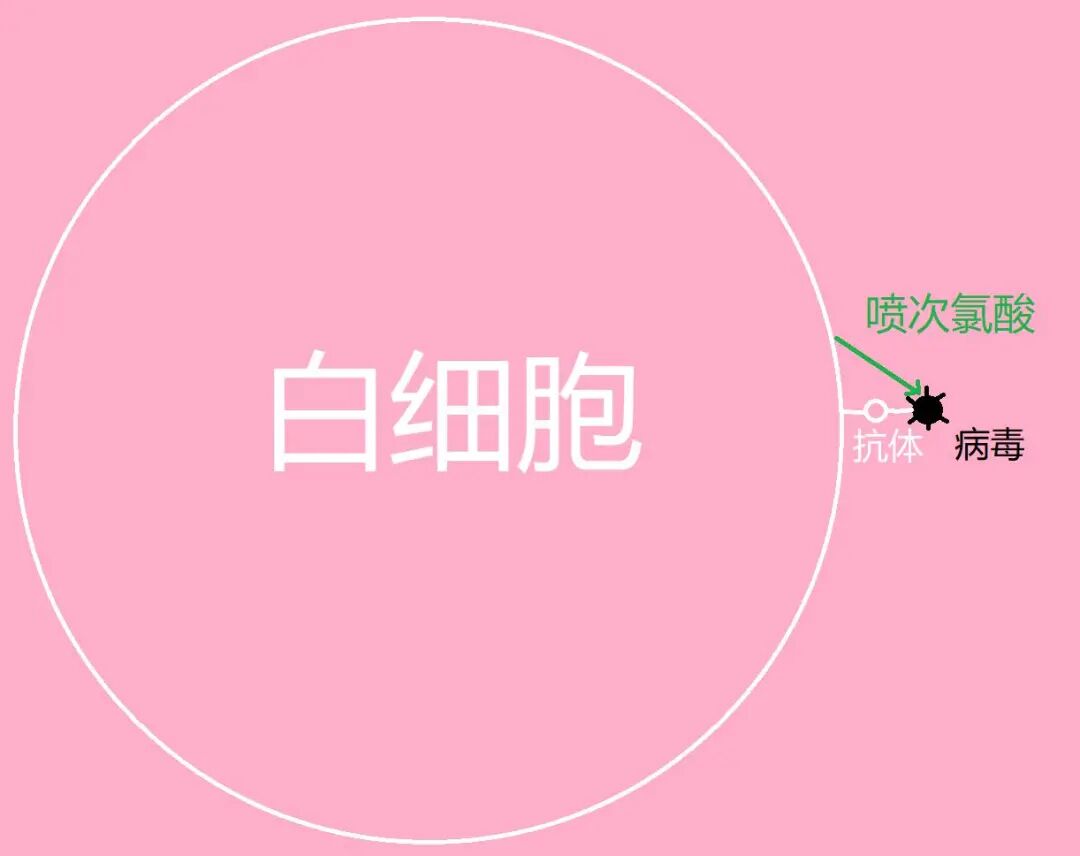
With antibodies: antibodies first stick to the virus, then immune cells stick to the antibody-virus complex, then secrete hypochlorous acid to kill the virus.
That's the principle. Without antibodies, your immune cells won't kill invading viruses. Even with hundreds of millions of viruses entering.
So — antibodies are key!
How do antibodies arise?
- "I work out daily, I'm muscular, my immunity is strong — I must have antibodies"
- "I practice TCM wellness daily, I'm full of righteous qi — I must have antibodies"
Sorry, none of these matter.
Antibody generation involves humoral immunity and cellular immunity. The details are numerous, but the general process:
- A virus enters the body and infects normal cells
- Before dying, normal cells metabolize viral characteristic protein molecules (antigens) to their cell surface
- Antigen presentation: via macrophages and dendritic cells, these strange proteins are presented to B cells
- B cells manufacture corresponding antibodies based on this viral characteristic protein
After B cells secrete antibodies, they circulate throughout the body, adhering to invading viruses and producing two effects:
- Antibody-antigen complexes (virus coated in antibodies) chemically react with and adhere to neutrophils, natural killer T cells, macrophages, and other immune cells. These immune cells secrete hypochlorous acid and other strong oxidizers to destroy the virus, or engulf it
- Once viruses are coated in antibodies, their spike proteins are blocked, hindering binding to human cell ACE2 channels
Blocking and killing — dual action. See how crucial antibodies are.
But different viruses require different antibodies. Among COVID variants, the original strain and Omicron have slightly different shell proteins, so antibodies from original strain infection bind less effectively to Omicron. Someone infected with the original strain, upon inhaling sufficient Omicron, can be reinfected.
Infecting viral load = (Inhaled viral load - Antibody quantity × Antibody efficacy) × Cell entry success rate
Knowing antibodies matter, how do COVID-naïve people acquire them? Must one suffer through infection?
Two solution pathways:
- Vaccine pathway: induce self-generated antibodies
- Antibody infusion pathway: introduce external antibodies
Vaccine pathway
Vaccines are weakened viruses manufactured in bulk — harmless or minimally harmful to humans, yet capable of activating immune responses and prompting B cells to produce antibodies. Common vaccine technology platforms include:
- Inactivated vaccines
- Adenovirus vector vaccines
- mRNA vaccines
With inactivated vaccines, weakened viruses that can't replicate enter the body, infect some cells, trigger an immune response, and B cells secrete corresponding antibodies. But since these weakened viruses don't replicate further, the damage is minimal. mRNA vaccines take a different approach: they introduce mRNA that encodes antigen proteins, which the body translates into those proteins, simultaneously activating both humoral and cellular immunity (inactivated vaccines only produce humoral immunity). From a technical standpoint, mRNA vaccine technology is more precise and has fewer side effects. However, it's not yet available on the mainland — domestic mRNA vaccines are still in clinical trials.
But once the immune response kicks in, B cells don't just keep cranking out COVID-19 antibodies indefinitely. After the first vaccine dose, if no new viral antigens enter the body, B cells move on to other tasks. And these antibody proteins have limited lifespans in the body — after a while, they're gone.
The immune system does have an interesting mechanism though: repeated infection with the same virus triggers an antibody explosion. With help from memory cells, B cells — seeing this same troublemaker keep showing up — produce more antibodies that stick around longer. After a second infection, detectable antibody levels in the body are higher and persist longer. That's why COVID-19 vaccines require at least two doses. If it's been a while since the second dose, you can get a booster shot. All of these increase antibody concentration in the body.
Of course, some viral vaccines provide long-lasting protection — the smallpox vaccine, for instance.
Another headache with SARS-CoV-2 is mutation. Since its emergence, we've seen the original strain, Alpha, Delta, and Omicron take turns causing trouble. When the virus mutates, surface antigen proteins change slightly, so antibodies triggered by different viruses or their corresponding vaccines aren't 100% cross-reactive. But they're not completely useless either. If targeted antibodies could stick to the virus 100% of the time, antibodies from different variants might only achieve 70% binding rates when encountering other strains.
The medical field's solution to this problem is multivalent vaccines. The "valence" refers to how many viral variants a vaccine can protect against simultaneously. The HPV vaccine familiar to many women also uses this "valence" concept — higher valence means protection against more viral variants. Hong Kong currently offers bivalent vaccines covering the original strain and two Omicron subvariants.
Mainland China's current vaccines are inactivated vaccines based on the original SARS-CoV-2 strain. The antibodies they produce don't bind to Omicron variants at 100% efficiency, but for mainland residents who can't access bivalent vaccines, they're still far better than nothing — at least for preventing severe disease.
So what does "prevents severe disease but not infection" actually mean?
Severe disease occurs when you have zero antibodies in your body. Only after the virus has massively destroyed cells do B cells start producing antibodies. By then, the virus has already replicated hundreds of billions of times and invaded the lungs. B cells finally produce antibodies, but lung cells have already suffered extensive necrosis — that's severe disease.
Timing is everything. Any antibodies in the body reduce how long the virus can run rampant, decrease the number of destroyed human cells, and crucially, block the virus from reaching the lungs in time — preventing severe disease.
Let me reiterate this infection rate formula:
Viral load reaching cells = (Inhaled viral load - Antibody quantity × Antibody efficacy) × Cell entry success rate
Setting aside the cell entry success rate for now, focus on antibody quantity and antibody efficacy:
- No vaccine: antibodies = 0
- Domestic vaccines: antibodies present but efficacy below 100%
- Multiple doses: maintain antibody quantity in the body
- Multivalent vaccines: increase antibody efficacy
As long as antibodies are present and inhaled viral load is low, that's what's called asymptomatic infection.
What protective measures to take should now be clear: get vaccinated.
There's also experimental evidence for why vaccines prevent severe disease but not infection. The Lancet recently published a paper where UK researchers found that nasal antibody concentrations are generally lower than blood antibody concentrations. If nasal antibodies are low but inhaled viral load is high, infection still occurs. But post-infection, blood antibodies are abundant, so the infection gets quickly suppressed — preventing severe disease. This highlights both how difficult COVID-19 is to prevent and the importance of nasal protection and nasal spray antibodies.
For elderly people and those with underlying conditions — should they get vaccinated? My suggestion: if you can avoid COVID-19 infection for the next six months, you might wait, as new medical breakthroughs may come soon. If infection risk exceeds 50% in the near term, better to get vaccinated with an attenuated or inactivated vaccine, or travel abroad for vaccination if possible.
Honestly, the human body fights invading viruses, bacteria, and parasites every day. The minor impact of vaccines is truly negligible.
However, in the days following vaccination, take strict precautions against viral exposure. If actual SARS-CoV-2 enters the body during this period, it places additional stress on the immune system.
Shortly after vaccination, when the immune response has activated and antibody levels are peaking, even inhaling small amounts of virus will be easily neutralized.
Based on my informal observations: in offices where 90% of people have been infected, the 10% who remain standing are those with proper protection who recently received booster shots. Of course, this is a small sample — take it as anecdotal.
Antibody infusion pathway
If infected people have antibodies, could we infuse their serum antibodies into me?
Recently there was news of a COVID-19 "super-donor" in the US with high concentrations of antibodies against various variants. People will naturally wonder: how can I get those antibodies too?
Antibody infusion is technically feasible. But we can't solve societal problems through recovered patient blood donations. The reliable route is factory-manufactured antibody proteins, such as monoclonal antibodies.
Once manufactured, these antibodies can't be made into pills because proteins get destroyed by stomach acid. Two delivery options remain:
-
Injection China's National Medical Products Administration has approved Brii Biosciences' neutralizing antibody combination therapy: amubarvimab (BRII-196) and romlusevimab injections. Clinically used for mild patients at risk of progressing to severe disease. However, these antibodies aren't Omicron-specific, and costs are relatively high.
-
Nasal spray SARS-CoV-2 invades through the upper respiratory tract, so nasal spray antibodies can effectively protect upper respiratory tract cells. "Recombinant fully human anti-SARS-CoV-2 monoclonal antibody nasal spray" is currently in clinical trials. Hopefully such products can solve efficacy and cost issues and reach market soon.
Summary: Step 2 — How to reduce viruses that reach cells
- For prevention, vaccination is the only viable option. Increase antibodies in the body to stick to viruses and let immune cells kill them before they invade cells.
- When hospitalized with potential progression to severe disease, doctors may administer monoclonal antibodies or serum from other patients.
At this point, let's revisit the first three elements of the human damage formula: Inhaled viral load - Antibody quantity × Antibody efficacy
Don't say "so-and-so got vaccinated and still tested positive, so vaccines are useless"; and don't assume that with antibodies, you can skip Step 1 protections.
- Inhale 100 viruses: intercepted by circulating antibodies, killed by patrolling immune cells — you're asymptomatic
- Inhale 100 million viruses: though hundreds of antibodies flow by every second, they're overwhelmed — many viruses successfully invade cells — you have symptoms
- Inhale 100 million viruses with no antibodies, waiting for B cells to manufacture them from scratch: the delay may allow lung infection — severe disease
So take both Step 1 and Step 2 seriously. Reduce inhaled viral load. Increase antibody levels in advance.
3. How to reduce viruses that enter cells
If SARS-CoV-2 evades antibody sticking and immune cell killing, it arrives at human cell membranes. Human cells have membrane barriers that don't let random substances through. Only organic molecules recognized as nutrients can cross. Unfortunately, SARS-CoV-2 can trick cells into thinking it's a nutrient.
That's just an analogy — cells and viruses don't think. It's actually a chemical reaction. Certain human cells have a surface protein called angiotensin-converting enzyme 2 (ACE2). SARS-CoV-2's outer shell has spike (S) proteins that can chemically bind with ACE2, using this channel to penetrate the cell membrane.
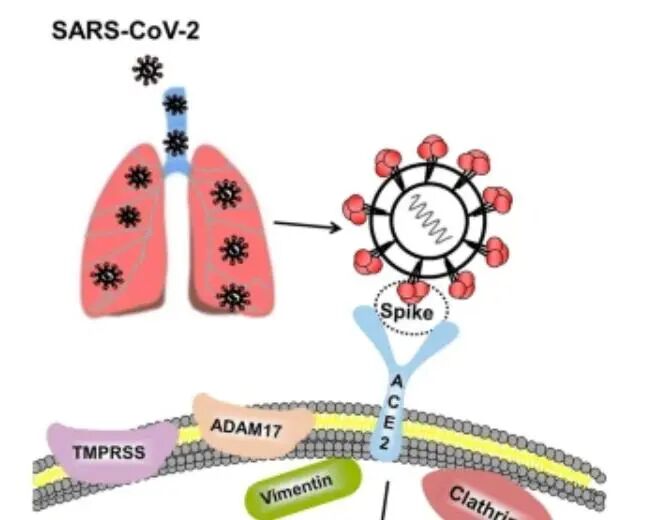
Image source: Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19
Not all human cell membranes have ACE2, of course. Immune cell membranes lack ACE2, so SARS-CoV-2 can't enter immune cells — otherwise we'd be in serious trouble. (Incidentally, HIV can attack immune cells.)
Besides ACE2, TMPRSS2 acts as a catalyst for viral entry through ACE2. The co-expression of both enzymes on cell membranes is concentrated mainly in the respiratory tract.
Understanding the mechanism naturally points to solutions: find ways to reduce ACE2 in respiratory tract cells.
Nature published a paper by Cambridge University researchers: FXR inhibition may protect from SARS-CoV-2 infection by reducing ACE2. They found in the lab that compounds Z-guggulsterone (ZGG) and ursodeoxycholic acid (UDCA) can downregulate ACE2, reducing susceptibility to SARS-CoV-2. Note that human clinical trials haven't started yet.
Interestingly, ursodeoxycholic acid is already an approved drug. But medication can only be taken short-term — we can't rely on daily drug use for COVID-19 prevention. And the long-term effects of ACE2 suppression on human health require further clinical data.
Curious readers might wonder: this angiotensin-converting enzyme 2 (ACE2) sounds related to vascular tension. Human blood vessels are elastic muscular tissue that can contract. Angiotensin causes vasoconstriction. ACE2 is the enzyme that converts angiotensin. We know that anger and stress narrow blood vessels, raising blood pressure. So does avoiding anger and stress help prevent COVID-19?
I was curious about this too and searched extensively — found no relevant evidence.
Because there's no evidence, I can only personally recommend relaxing, not getting angry, stressed, or anxious, letting your respiratory tract cells be at ease.
Oh, and if you want respiratory tract cells to be comfortable, pay attention to several air quality indicators:
- Temperature: above 20°C
- Humidity: above 40%
- Oxygen concentration: between 20.5% and 23%
- No other harmful gases
Winters in northern China are cold and dry — prime conditions for respiratory illness. If your radiator isn't cutting it, don't skimp on electricity for air conditioners or space heaters. A decent humidifier is also a worthwhile investment for quality of life.
I'm a data nerd, so I monitor all the air metrics above with professional instruments. But oxygen and harmful gas concentrations rarely go out of range. For most people, the simplest and most effective step is putting a thermometer-hygrometer by your bedside. Those eight hours of sleep are critical — if you're spending them at the wrong temperature and humidity, getting sick becomes much more likely.
Once a virus enters a cell membrane through ACE2, its next target is usually the cell's nucleus. But RNA viruses like SARS-CoV-2 don't need to wait — they can start replicating using the cell's nutrients right away. A single virus is so small it's practically invisible in diagrams of cell interiors.
Human cells do have defense mechanisms to destroy viruses, but this gets fairly academic, and critically: humans have no way to intervene. It's purely genetic, and genetic variation among humans is actually quite small. So I won't go deep into intracellular defense details here — interested readers can check out the documentary Curiosity: The Cell at War.
But we do need to cover some key information about how viruses invade the nucleus, such as where antibodies come from.
When a virus enters a cell, it needs to unpack its protein shell so the RNA inside can start replicating. At this point, the viral protein shell gets expelled to the cell membrane surface by the cell's metabolic system — cells have a purification mechanism for getting rid of unwanted material.
Normally, human cells absorb nutrients from blood (oxygen, glucose, fats, amino acids, vitamins, etc.) to fuel mitosis, turning one cell into two. But viruses redirect all these nutrients to replicating themselves — both the inner RNA and the protein shell — manufacturing vast quantities and assembling identical copies.
Within dozens of hours, the cell becomes packed with tens of thousands of viruses and dies. These viruses burst from the ruptured membrane and begin infecting surrounding cells.
But remember that earlier step? Before entering the nucleus, the viral protein shell disassembles — and these shells get pushed to the cell membrane surface. This is where immune response kicks in:
- First, patrolling immune cells notice: hey, why are there all these weird proteins piled on this cell's surface? This cell isn't normal. If multiple cells show these strange proteins, many cells are abnormal.
- Through coordination between macrophages and dendritic cells, these strange proteins get presented to B cells — this process is called antigen presentation.
- B cells begin manufacturing antibodies based on the antigens.
If antibodies already exist in the body, they'll stick to the viral shells on the cell surface. Then the immune system's attack specialists — neutrophils, natural killer T cells, macrophages — will kill this antibody-coated human cell. Yes, they kill your own cells. This prevents the virus from replicating and spreading.
If there are no antibodies, if too many cells are infected, or if immune response is slow, the virus quickly explodes.
Bacterial reproduction is doubling: one becomes two, two become four, four become eight, eight become sixteen... already scary enough. At one million, doubling means two million.
But viral replication puts bacteria to shame. Viruses replicate ten-thousand-fold. One virus becomes ten thousand, ten thousand become one hundred million, one hundred million become... the math gets unwieldy.
Under this explosive reproduction, timing is everything. The sooner the immune system activates, the more symptoms can be controlled. The later, the more severe they become.
Summary: Nuclear entry success rate is very difficult to influence. Reducing ACE2 receptor expression remains purely theoretical. So frontline protection remains key: reducing viral inhalation, boosting antibodies, and physically clearing infected cells from the nose and throat.
4. The Fierce Battle
When the host cell dies and tens of thousands of COVID-19 viruses burst free, the virus sounds the horn for large-scale offensive. These viruses march down the respiratory tract, layer by layer — from nose, pharynx, larynx, trachea, to lungs.
But unfortunately, without antibodies, the immune system's attack specialists remain silent, watching the virus ravage and infect healthy human cells. Only after B cells produce antibodies do immune cells begin counterattacking, and the tug-of-war truly begins. Everything before this is the incubation period.
Though you can't see how immune cells and viruses battle inside you, you'll gradually feel the manifestations: nasal congestion, dry throat, sore throat, body aches, fever, smell disorders, shortness of breath...
4.1 Dry Throat
In early disease stages, nasal congestion, dry throat, and sore throat arrive in succession. Contrary to what most people think, viruses don't stimulate your pain nerves. You don't feel pain when respiratory cells die from viral infection.
If you've been vaccinated, you'll have antibodies against the original strain. With these antibodies, immune cells will continuously eliminate some viruses, just less efficiently. Without them, things get truly bad.
But even vaccinated, if you've reached this symptomatic stage, it means you inhaled too many viruses — original strain antibody concentrations are insufficient. What's critical now is that B cells begin secreting Omicron-specific antibodies.
After receiving viral antigens presented by dendritic cells, B cells begin secreting large quantities of Omicron antibodies, which circulate throughout the bloodstream.
At this point, we need to understand: the blood system and respiratory muscle system are different. Infected cells are in the respiratory tract; antibodies and immune cells are in the blood. What to do?
Blood vessels near viral concentrations dilate, their walls thin, and blood flow slows — this makes it easier for antibodies and immune cells in the blood to cross the vessel walls and attack. For example, when throat surface cells are heavily infected, throat blood vessels dilate, making the throat appear red and swollen. This is the mechanism of inflammation.
The white blood cells in the image are immune cells.
People who don't understand pathology mistakenly think throat redness and swelling is the disease itself, and try taking medicine to reduce inflammation. They don't realize throat redness is the immune system treating the disease — once the virus is eliminated, inflammatory signs naturally subside.
Similarly, mistaking symptoms for root causes — besides anti-inflammatories, there's fever reduction, cough suppression, decongestants, anti-nausea, anti-diarrhea. I collectively call these the "Humanity's Baffling Behaviors: Not Understanding Pathology" series.
Coughing and sneezing are respiratory tract evolutionary mechanisms for expulsion.
- When foreign matter is in the nasal cavity, sneezing ejects it.
- When foreign matter is in the trachea, coughing ejects it.
If you can spray out viruses, that's a wonderful thing — it dramatically reduces pressure on immune cells. Sneezes generate wind speeds exceeding force 10, and a single sneeze or cough can expel tens of thousands of viruses, significantly lightening the immune load.
Of course, promptly disinfect the expelled air with alcohol spray to avoid re-inhalation or infecting others.
Additionally, nasal rinsing and phlegm clearing remain effective physical methods for expelling viruses or infected cells.
Some patients feel nauseous after COVID-19 infection, also from throat discomfort — if you need to vomit, go ahead.
Gargling is theoretically useful too. Physically flushing throat surface viruses and infected cells into the stomach, where hydrochloric acid in gastric juice kills them. But gargling works best when antibodies are present in the body. While SARS-CoV-2 doesn't infect stomach cells, it does infect intestinal cells — without antibodies, opening the pyloric sphincter to let many through could cause trouble.
If you're unvaccinated and experiencing first infection, my advice to drink more warm water comes after fever sets in.
When your throat is uncomfortable, be careful not to take random medications.
Anti-inflammatory drugs are antibiotics — amoxicillin, cephalosporins, etc. They kill bacteria, not viruses. Their mechanism inhibits bacterial cell wall synthesis, and viruses have no cell wall to begin with.
Unless you discover concurrent bacterial infection, don't take antibiotics. Even with concurrent ordinary flu, don't take antibiotics. Influenza and colds are caused by viruses, unrelated to bacteria.
Cough suppressants should also be used cautiously — dextromethorphan, for example, mainly suppresses the cough center in the medulla. Though if coughing prevents sleep or causes significant respiratory damage, these extreme reactions should also be avoided.
Additionally, thick winter comforters easily breed dust mites, and inhaling these microorganisms can also trigger coughing. Watch out for these external causes worsening your condition.
4.2 Fever
Immune cells kill three things:
- Antibody-coated viruses
- Virus-infected cells
- And surrounding healthy cells
Yes, once battle commences, immune cells go on a rampage, killing healthy cells around infection sites to prevent viral expansion. Because when no living cells remain around the virus for it to infect, self-replication stops.
But each immune cell's capacity to kill these three things is limited. Immune cells, also called white blood cells, have many subtypes. The main pathogen-killing forces include: neutrophils, natural killer T cells, macrophages, etc.
Rough estimate: one immune cell can kill on the order of tens of thousands of viruses, or several dozen cells. This is hand-to-hand combat — viruses, human immune cells, and infected normal cells all suffer massive casualties.
- Negative factors: viral load, replication speed.
- Positive factors: antibody production speed, immune cell numbers, per-cell killing efficiency.
The human body actually has plenty of immune cell reserves, and the kill rate per immune cell can be boosted. Want to guess how? Fever.
The immune system has a pyrogenic mechanism. When immune cells get overwhelmed fighting viruses, EP-class cells release pyrogens like prostaglandins and interferons. Both prostaglandins and interferons stimulate neurons, triggering pain. That pain is essentially the immune system teaching you a lesson — a reminder to take better preventive care next time instead of putting your immune system through this ordeal.
As neutrophils and macrophages circulate throughout the bloodstream, prostaglandins and interferons end up everywhere, causing whole-body pain. Interferons also cause headaches and fatigue. But their main purpose isn't punishment — when these chemical hormones accumulate in sufficient quantities, they signal the brain's command center to raise body temperature. The more they build up, the higher the fever.
Why raise temperature? To activate immune cells and suppress viral activity. At higher temperatures, immune cells become more efficient at killing viruses, infected cells, and surrounding compromised cells. Viruses are heat-sensitive too — while this temperature won't kill them outright, it does dampen their activity.
So pay attention here: think twice before taking fever reducers!
Both ibuprofen and aspirin are NSAIDs (non-steroidal anti-inflammatory drugs). Their mechanism works by inhibiting the prostaglandin synthesis mentioned above. Less prostaglandin means less neuronal stimulation, so the brain doesn't raise body temperature — pain relief and temperature reduction in one tidy package. Sounds great.
Except the virus isn't dead. Ibuprofen doesn't kill viruses, and by blocking the temperature rise, it actually suppresses immune cell killing efficiency. The virus survives, so the immune system keeps secreting prostaglandins and calling for higher temperatures. Some people take ibuprofen, their fever and pain subside superficially, then return when the drug wears off — a frustrating cycle.
For healthy adults, just let the fever run its course. Bundle up in blankets to help raise body temperature — you're fighting alongside your immune system.
Will fever damage your brain? Baidu Baike states this clearly:
Can high fever damage the brain? Currently there's no evidence that fever itself causes neurological damage. However, fever increases central nervous system excitability. Especially with high fever, children may become irritable, delirious, or experience hallucinations. Because children's nervous systems are not yet mature, fever during infancy is more likely to trigger febrile seizures than at other ages.
So you only need to physically cool a child's head with a wet towel if their temperature exceeds 39°C (102.2°F). Use a forehead thermometer to monitor. If the wet towel stops working, promptly loosen clothing to help dissipate heat. The goal is precise temperature control around 39°C.
Incidentally, children's COVID symptoms are generally mild. Among people I know, the ones who suffered through days of recurring pain and fever were all grown men.
Of course, sometimes the immune system overreacts. If you hit 40°C (104°F), you do need to reduce the fever — beyond that, heat stroke becomes a risk.
Note: this article is not advising readers to avoid fever reducers entirely. Everyone's pain tolerance differs, and people pursue different definitions of wellbeing. This article simply explains the mechanisms. Understanding the principles, you can make your own informed choices.
Since fever reducers don't kill COVID, what does?
Only two drugs have received clinical approval in China for actually killing COVID: the imported drug Paxlovid and the domestic drug Azvudine. (This excludes monoclonal antibodies and convalescent plasma that doctors may administer in hospitals.)
-
Paxlovid
-
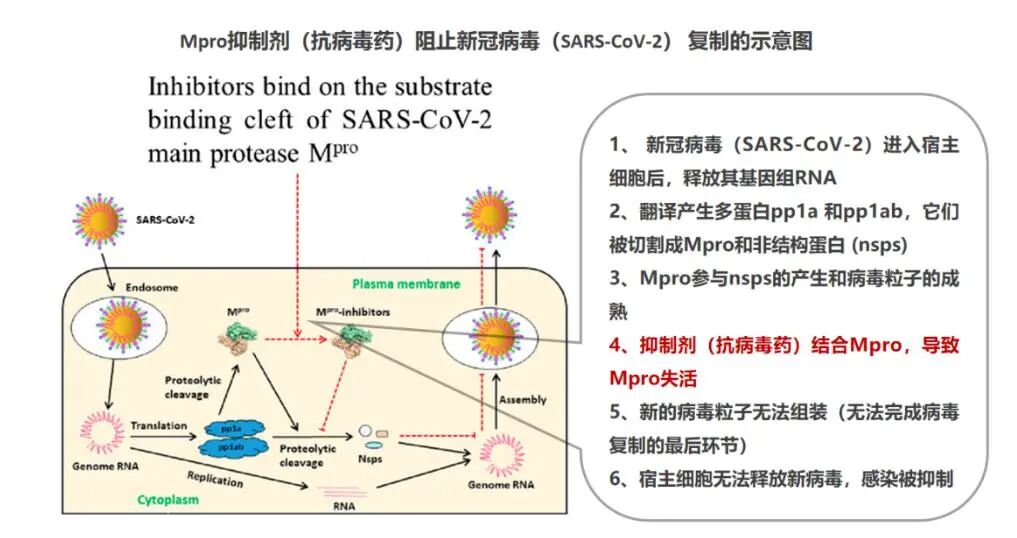
Its mechanism targets and disrupts the COVID virus's replication process. "Targeted" is a medical term meaning it destroys the pathogen directionally without harming other human cells.
-
It actually consists of two drugs: Nirmatrelvir and Ritonavir.
-
Nirmatrelvir is the key component — a protease inhibitor. When it encounters the virus, it deactivates the virus's Mpro site. Any virus that binds to it becomes unable to self-replicate.
-
Ritonavir's role is inhibiting liver metabolism of Nirmatrelvir, keeping Nirmatrelvir active in the body longer.
-
Domestic Azvudine
-
It was originally developed to treat HIV. It is not a targeted COVID inhibitor.
-
This is the pharmaceutical company's officially published paper: Azvudine (FNC): a promising clinical candidate for COVID-19 treatment
-
Clinical trial data is scarce. Double-blind test results and side effects are poorly known. No evaluation for now.
As for other drugs — whether Western medicine, traditional Chinese medicine, or folk remedies — none have passed COVID clinical trials: large-scale, controlled-condition, double-blind testing. If any of their effectiveness were clinically proven, they would naturally be added to the list above.
Social media is full of well-meaning "worked for me" recommendations, but a drug or treatment protocol only yields valid conclusions through large-scale double-blind testing. For a self-limiting disease like COVID, far too many people love to steal credit from the immune system. Your immune system is fighting desperately for you, yet because you don't understand it, you place faith in various unreliable tricks you've "personally tested."
Dr. Zhang Wenhong's advice for COVID patients: Turn off your phone, sleep, drink plenty of water, take vitamins. The logic is simple — most people just don't believe it.
Of course, high-risk groups need antiviral drugs. And they need them promptly. If you wait until lung cells have already died in large numbers, it's too late. So for elderly people and those with high-risk comorbidities, don't wait for antigen test results once infected. At the first symptoms of dry throat and fever, go to the hospital immediately and ask your doctor for Paxlovid.
Regarding pain, approach it calmly — it's part of your life. Much of what people experience as pain is actually pain plus fear. They become extremely anxious, convinced they're going to die, take random medications, and折腾 themselves into additional illnesses. Fear comes from the unknown. If people understood nervous system mechanisms, they'd have deeper comprehension of pain. Then during pain, there would only be pain itself — no fear triggered by the unknown.
For COVID, if you clearly understand the mechanisms of pain, accept the lesson willingly, and support your immune system's fight, you'll feel much better.
4.3 Shortness of Breath
If you've reached shortness of breath, the virus has already invaded the lungs in large numbers. Lung cells are responsible for absorbing and filtering oxygen for delivery to the bloodstream. If lung cells die, blood oxygen drops. Every organ in the body depends on the blood system to deliver oxygen. Whether it's brain function, limb movement, or cell division and growth — all require oxygen.
For the brain, oxygen deprivation is far more serious than fever. Brain cells cannot regenerate. If they die from oxygen deprivation, they're gone.
Normal blood oxygen concentration is 95–97%. Below 92% is warning territory. If you feel short of breath, test blood oxygen promptly. Ideally, start monitoring blood oxygen during the fever phase itself. Blood oxygen monitors are inexpensive — around 100–200 RMB suffices.
When oxygen is low, oxygen inhalation is the first priority. Oxygen canisters are cheap too — several dozen RMB per bottle. Professionals can also prepare ventilators at home — several thousand RMB. For non-professionals, go to the hospital promptly.
Beyond blood oxygen, several other indicators can track disease progression. The latest COVID-19 Diagnosis and Treatment Protocol (Trial Version 9) lists these:
- Tissue oxygenation indicators (such as finger oxygen saturation, oxygenation index) deteriorating or progressive lactate elevation
- Peripheral blood lymphocyte count progressively decreasing, or inflammatory factors such as interleukin-6 (IL-6), CRP, ferritin progressively rising
- D-dimer and other coagulation function-related indicators significantly elevated
- Chest imaging showing obvious progression of lung lesions
But these indicators are difficult to self-check without hospital access. The most accessible option for ordinary people is still buying a blood oxygen monitor.
Additionally, several observable signs in children are important: increased respiratory rate, poor mental responsiveness, lethargy. If these appear, go to the hospital promptly.
How do doctors treat hospitalized severe patients? Management of other underlying conditions is beyond this article's scope. For COVID specifically, the National Health Commission's guidance to hospitals includes:
- Paxlovid antiviral: blocks viral replication
- Monoclonal antibodies: amubarvimab/romlusevimab injection. Injected antibodies neutralize the virus. However, these antibodies are not Omicron-specific.
- Intravenous COVID-19 human immunoglobulin
- Transfusion of convalescent plasma from recovered patients — another method of externally inputting antibodies
- Ventilators, extracorporeal membrane oxygenation (ECMO)
Some severe patients suffer from excessive immune response — cytokine storm. The virus replicates too fast, the immune system goes into overdrive, regulation fails, and it kills the body's own vital organ cells. In these cases, doctors suppress the immune system with glucocorticoids like dexamethasone.
However, Omicron's replication speed in the lungs is far lower than the original strain. Reports of cytokine storm are rare.
5. Recovery and Long-Term Effects
For healthy people, fever typically lasts only 1–2 days. The human immune system is remarkably powerful — a complex, robust system refined over tens of thousands of years of evolution. Once immune response initiates, B cells secrete antibodies with ferocious speed, and bone marrow stores countless reserve white blood cells that all enter combat.
Fever reduction simply means immune cells no longer need elevated temperatures to boost killing efficiency. Recurring fevers are generally caused by taking fever reducers that treat symptoms while suppressing the root cause.
Of course, if you're truly unfortunate, renewed fever could mean infection with other bacteria or viruses — though probability is extremely low.
The subsequent recovery process is battlefield cleanup. White cell corpses, infected cell corpses, viral corpses — they pile up like mountains. Cleanup relies on macrophages and coughing. Macrophages engulf these remains; coughing also serves to clear debris. If you take cough suppressants, cleanup simply proceeds more slowly — macrophages will eventually finish regardless. Unless coughing affects sleep, there's no need for cough medicine. Once the debris is cleared, coughing stops naturally.
Whether during illness or recovery, environmental disinfection should remain a constant priority:
- Wash clothes and bedding in high-temperature washing machines or dryers
- Disinfect daily necessities in sterilization cabinets
After sweating, replenish electrolyte water. Simple electrolyte water can be homemade: lemon + salt + sugar water.
The hundreds of millions of dead cells need nutrients to regenerate. Supplement with carbohydrates, protein, and vitamins. Though if you want to lose weight, this is actually opportune — nutrients for new cells can come from the fat beneath your belly. Just ensure adequate vitamin supply.
The human body is an exquisitely refined system with various risk reserve protocols. Not so easy to die, yet not so easy to enhance either. Many people live entire lifetimes without learning to coexist with the tens of trillions of cells in their body. Only by truly understanding them can you better protect yourself.
Long COVID
Based on overseas statistics, some people experience lingering effects lasting several months: COVID brain fog. Manifestations include:
- Memory impairment
- Difficulty concentrating
- Slowed reaction times
Some people also experience loss of smell during the acute phase. While these issues are more common in severe cases, they can occur in mild infections too. According to data from a Nature paper, "Looking for lights in the fog of long-term neurological COVID," roughly 7% of people develop what we call long COVID.
The mechanism behind long COVID remains unclear. Theoretically, SARS-CoV-2 cannot infect nerve cells that lack ACE2 receptors. The leading hypothesis is that it's caused by immune-mediated neurological inflammation. Fortunately, these symptoms typically resolve within several months.
Reinfection
As for reinfection — what the author calls "re-yang" (testing positive again) — the same infection formula still applies:
Infectious viral load = (Inhaled viral load - Antibody count × Antibody efficacy) × Cell entry success rate
After recovering from a first Omicron infection, you do develop Omicron-specific antibodies, but these antibody levels decline over time. When antibody levels are insufficient, you still need to reduce your inhaled viral load — otherwise, reinfection occurs.
Similarly, after catching one Omicron subvariant, inhaling a large dose of a different subvariant later on can also lead to reinfection. So don't get cocky after recovery.
Summary
Let's revisit the formula from the beginning:
Degree of bodily harm from virus = (Inhaled viral load - Antibody count × Antibody efficacy) × Cell entry success rate × Latent-phase infected cell clearance rate × 10,000 - Immune cell combat effectiveness - Antiviral drug suppression effect
- Inhaled viral load factors: Mask-wearing, social distancing, hand washing, environmental disinfection, nasal rinsing, throat clearing
- Antibody count factors: Immune activation through infection or vaccination; secondary activation triggering antibody surge; antibody levels decline over time since immune response
- Antibody efficacy factors: Similarity between the immune-triggering strain and the infecting strain
- Cell entry success rate factors: ACE2 receptor concentration. Non-clinical papers suggest ursodeoxycholic acid may suppress ACE2
- Latent-phase infected cell clearance rate factors: Nasal rinsing, throat clearing, pre-existing antibody count and efficacy
- Immune cell combat effectiveness: Total immune cell count is generally sufficient; individual cell combat effectiveness correlates with body temperature — higher temperature means stronger individual performance. Additionally, improper environmental temperature and humidity increase immune system burden
- Antiviral drug suppression effect: Paxlovid currently has clear supporting data; azvudine has passed clinical trials but data is unavailable; other drugs lack clinical validation
Admittedly, subtracting those last two terms directly isn't mathematically rigorous, but the underlying principle holds.
Another factor is the speed of immune response activation after cell infection — how quickly effector antibodies can be produced. Faster is better, but this is largely a fixed parameter, so it's not worth worrying about.
Virus and immune system exist in a zero-sum dynamic. Many links in this chain are beyond human control. For prevention, the most basic, feasible, and cost-effective measures boil down to just three:
- Reduce inhaled viral load
- Get vaccinated to increase antibodies
- Maintain proper environmental temperature and humidity
For those already infected with a typical case, the to-do list is similarly short:
- Rest more
- Drink plenty of warm water
- Supplement vitamins and electrolytes
- Maintain appropriately elevated body temperature to suppress viral replication
- Keep surrounding temperature and humidity optimal
- Rinse nasal passages and clear throat
This summary may disappoint some readers — after tens of thousands of words, the conclusion is just these few bullet points? But the real purpose of this article was never simply to tell you these things. It was to help you understand your body:
- Know how your immune system guards your health
- Know what helps it and what harms it
- Know how it punishes you when you harm it
- Learn to distinguish what's effective from what's misinformation.
If it can also help you develop a scientific framework for analyzing other problems in the future, that would be even better.
Let's fight COVID based on first principles. Protect your body by understanding it first — then stand shoulder-to-shoulder with the tens of trillions of cells inside you to defend your health!

Image from the manga Cells at Work! Code Black. From left to right: centrophil, natural killer T cell, and macrophage in anthropomorphized form.
Author's note: I am not a professional content creator and am not skilled at image selection and layout. Others are welcome to refine and republish this article. No copyright — feel free to share freely.